Tags
awesome, interviews, minneapolis, present day, real life, research
These are not quite half of the wonderful reasons I haven’t been writing (except e-mails and letters).
Thought maybe you’d like to see.

08 Monday Jul 2013
Posted in Present Day, Real Life
Tags
awesome, interviews, minneapolis, present day, real life, research
These are not quite half of the wonderful reasons I haven’t been writing (except e-mails and letters).
Thought maybe you’d like to see.
27 Thursday Jun 2013
Posted in Kenny Institute, Society
Tags
“‘Bill’ Stanley William / Willis Bell (??)”
That name is written not far beneath Elizabeth Kenny’s, in my roster of important figures in this absurdly crowded story. So far, I’ve talked only about Kenny herself, and about her patients—and, in my last post, about myself—but there are dozens, if not hundreds, of others who figure into this story. They are nearly as vibrant and dynamic as its central character, but were afforded nowhere near as much press coverage, and finding ways to get to know them has proven both delightful and infuriating.
This story is vast, almost beyond my ability to see it all at once, force a wide and ever-changing vista into a single frame. It’s yet another part of what I love about it: its enormity, and the delight I take in the knowledge that each one of the many thousands of people who passed through the Kenny Institute, for a week or a month or a year, came away with a different impression of what the place was and exactly who the people were that lived and worked there.
Because it’s not what a thing really is that we see, that we remember. It’s what it means to us.
The physical therapist with that heavily annotated name is one of my favorites: one of the most interesting, and so far one of the most enigmatic. It isn’t just that the names on his paperwork don’t match up (though they don’t, always, with William/Willis the main point of contention). It’s that he seems to have used different names with different people—and it’s that one small quirk that has me curiously transfixed.
It was while I was talking to my interviewee Russell, who fell ill in the summer of 1940, that I figured this out: I’d asked him about the people who cared for him other than Kenny, hoping to draw out some of the names I already knew. “[S]he had one male and one female nurse that was on her staff, Australians,” he said, but he couldn’t remember their names.
The girl was probably Mary, I told him, or else Valerie: Kenny’s adopted daughter and protégé, and her favorite physical therapist, respectively, both of whom accompanied her from Australia. The boy’s name was almost certainly Bill, another therapist she’d trained—someone I’d heard stories about, who all of the kids seemed to adore. I’d read a lot about Bill, and I was confident that this was Russell’s guy. Did any of that sound familiar? I asked.
It didn’t. Not then. But a few minutes later, he told me about this “orderly” he’d worked with almost constantly, someone who helped him with his treatments and carried out his exercises. Stan, he said, thoughtlessly. Sliding out, the way things do, from dark corners of memory too cluttered to retrieve anything from when you rifle through them in the light.
And something went off in my head.
Stan. Stanley? Stanley William? Bill?
I’d read people’s recollections about the somewhat unfortunately named Bill Bell, but never any—at least, none that I recall—about Stan. And yet it’s obvious that the man Russell spoke of with such mischievous warmth in his voice was the same one who’d watched over so many others in their most fragile and brilliant moments: outgoing and deadpan and subversively indulgent, with the same Aussie drawl Kenny had.
Stanley et cetera Bell was one of the Kenny Institute’s first staff members—he started working for Kenny in the States in 1940, and the Institute wasn’t dedicated until December of 1942—and to all appearances one of its most beloved. Kenny summoned him from Australia the instant she was ensconced in Minneapolis; she had trained him in physical therapy at a clinic she ran in Queensland, and the two had worked closely together for his entire career to date. As apparently skilled and authoritative as anyone else on Kenny’s staff, Bill/Stan also had a bit of a “good cop” reputation, contrasting with the women’s more severely expressed expectations. “Stan and I got along like a million bucks,” Russell told me, grinning, and it was clear that to a lost, lonely kid looking for guidance, that meant everything.
 The Kenny Institute, as it was in the 1940s, was, and still sometimes is, accused of being a “cult of personality”—but no hospital serving nearly a hundred people as long-term inpatients, and two or three times that during certain epidemic swells, could operate on the strength of a single individual, no matter how formidable she might have been. Sister Kenny’s ethos permeated the place, but it’s the auxiliary staff former patients recall most vividly: the people they saw every day, sometimes more than once. (Sometimes an exasperatingly large number of times.) The nurses. The “packers” who swathed their bodies in hot wool blankets to ease their cramps. And the therapists, who coaxed them so slowly and steadily back to life. People who knew them better than they knew themselves, at least for that brief breath-held moment in time, who bore witness to their tears and shared in their triumphs, and were both the cause and the cure of their pain.
The Kenny Institute, as it was in the 1940s, was, and still sometimes is, accused of being a “cult of personality”—but no hospital serving nearly a hundred people as long-term inpatients, and two or three times that during certain epidemic swells, could operate on the strength of a single individual, no matter how formidable she might have been. Sister Kenny’s ethos permeated the place, but it’s the auxiliary staff former patients recall most vividly: the people they saw every day, sometimes more than once. (Sometimes an exasperatingly large number of times.) The nurses. The “packers” who swathed their bodies in hot wool blankets to ease their cramps. And the therapists, who coaxed them so slowly and steadily back to life. People who knew them better than they knew themselves, at least for that brief breath-held moment in time, who bore witness to their tears and shared in their triumphs, and were both the cause and the cure of their pain.
It was the most intimate relationship many of them had ever had—not just the children, but, by all accounts, many of the adults as well. It amazes me how openly Kenny patients talk about their doctors and therapists—not just in retrospect, but in things they wrote while they were still in the hospital, or shortly thereafter. They seem to have talked to them just as candidly: without any of the frightened reverence I’m used to seeing in the face of such an authority gap, they tease and question them even as they look to them for guidance. It’s respect, and well-earned, not intimidation.
It’s like I wrote in the last post: this is real life. With all of the extraneous distraction, and all of the social nicety, stripped away. If you didn’t have the luxury of hiding from it, it was good at least to have someone with whom to share, and these were the people they could trust. And the patients—some of them, anyway, when they were ready—plunged into this highly unusual dynamic with an abandon and a sense of freedom they didn’t seem to feel anywhere else. You weren’t supposed to talk about it—about polio, about your fears, about much of anything at all; recollections of interactions with family and friends frequently emanate squirming discomfort. But this specific relationship, between the Kenny patients and their therapists, that you might expect to be so fraught with expectation and fear, is both ocean-deep and light as air.
And they entrance me, coming to life on these old and crinkled pages. It’s uncanny, in a way, to come away with such a strong impression of an individual—not just the mysterious Mr. Bell, but so many of these people, the ones who show up all the time and the ones I’ve “met” just once or twice—without actually knowing anything about them. I have a copy of a card with Bell’s credentials on it—but most of Kenny’s resume was faked, so I have a hard time believing his is wholly straightforward. He spent some time in the military starting in 1945, but how that came about, and why, as far as I can tell, he never returned to the Institute, remains a mystery. He was married, with at least two children, but I don’t know anything about his family besides that they existed.
 The only thing about Bill/Stan Bell I don’t have any trouble figuring out is why he was so thoroughly beloved. The first story I ever read about him was relayed by a man named Robert Gurney, in an interview for the book Polio’s Legacy. Robert called him Bill. He called him Bill, and he spoke about the winter of 1940, and learning to walk again: seventeen years old at the time, Robert insisted he couldn’t do it, but his technician felt otherwise. After a couple unsteady laps around the therapy table, Bill announced that Robert, with Bill’s help, was going to walk back to his room. This plan seemed difficult to protest, so off they went, until one of Robert’s friends noticed him walking alone and called out congratulations; as it turned out, Bill had stopped to “[talk] to a couple of pretty nurses,” and Robert had inadvertently kept going without him. As soon as he realized what had happened, Robert promptly wavered and fell, but he tells it as a deeply happy story, infused with nostalgia, tinged with gratitude.
The only thing about Bill/Stan Bell I don’t have any trouble figuring out is why he was so thoroughly beloved. The first story I ever read about him was relayed by a man named Robert Gurney, in an interview for the book Polio’s Legacy. Robert called him Bill. He called him Bill, and he spoke about the winter of 1940, and learning to walk again: seventeen years old at the time, Robert insisted he couldn’t do it, but his technician felt otherwise. After a couple unsteady laps around the therapy table, Bill announced that Robert, with Bill’s help, was going to walk back to his room. This plan seemed difficult to protest, so off they went, until one of Robert’s friends noticed him walking alone and called out congratulations; as it turned out, Bill had stopped to “[talk] to a couple of pretty nurses,” and Robert had inadvertently kept going without him. As soon as he realized what had happened, Robert promptly wavered and fell, but he tells it as a deeply happy story, infused with nostalgia, tinged with gratitude.
“Henry [the friend] was laughing so hard he was crying,” Gurney says, “and I was just sitting on the floor laughing. But from then on, I walked.”
The interview is eight or nine pages long, and only one of them deals with this incident, much less Bill himself. But I came away from those bare sentences with a distinct impression of who this person was and how he thought (though I still can’t decide whether the detour to chat up the nurses was an actual lark or just a ruse). I feel like that’s the opposite of what usually happens, like I’m getting to know these people inside out: it’s so easy to accumulate semantic details about a person—what do you do, where are you from, where’d you go to school?—and so hard to actually learn anything about who they are. But these people come across as so raw, so earnest, so inside-out, that it’s hard not to see them right away. You see them in their letters, in their memos, in the stories that others tell about them, so enthusiastic and conspiratorial: the way they really were, in the day-in and day-out of a job both unforgiving and unfathomably rewarding.
That’s why I’m so curious about the name change. About why Russell talks about Stan, and Robert reminisces about Bill, when they met him the very same summer, a span of time in which you expect there to be a united front. Maybe it’s an odd thing to have latched onto so tightly, and with such insistent curiosity. But names have a literally mythological power, and changing them is more than just semantic, because your name tells you—you, not just the rest of the world—so very much about who you are. You can be a different person, with a different name. Even if they both belong to you, and neither one is a “disguise.”
I know because I changed my name, a little less than a year ago, one little piecemeal introduction at a time, from something that merely belonged to me to something that was mine. I’d been Tori since I was born, an abbreviation of a given name I claimed to hate, and that even my parents never meant to call me aloud: too regal, too stuffy. I was so stubborn about it that it says Tori on my university diploma. But about a year ago, with the world swirling around me, I started wondering if that was the person I felt like—or the person I wanted to be. I started wondering about Tori on the cover of a book. And then, one day, with a small and instantaneous thrill of transgression: Hi. I’m Victoria.
I love this “new” name. Victoria is who I chose to be. And there are many people in my life now who know me only that way: when my yoga teacher Matt calls me out in class, it is Victoria he gently chides; Victoria is the name at the top of this page. It startles me when I swipe my loyalty card at the chain café I’ve eaten at practically every other day since I was a teenager, and when my order comes up they call out, “Tori?” And yet, sometimes, for reasons I can’t even fathom, a department store salesperson will ask my name, and I’ll chirp the shorter version—not because I forget, for a moment, but because it feels more appropriate. Even though most of the time I cringe, unfairly, when I see that worn-out word, the old name, a relic of a person I’m relieved to no longer be.
Sometimes a name is just a name. But sometimes it’s a threshold.
So that’s a moment—a pair of them, in fact—I wish I somehow could have witnessed: whatever the space was between Stan/Bill’s two introductions, and whatever spontaneous impulse triggered the change. Maybe different people seemed to need different things. Maybe different contexts brought different levels of comfort. Maybe he was still trying to figure out who he was going to be in the U.S., and whether that was any different from the person he had been back in Australia. Maybe it’s nothing. Maybe he went by both names as a matter of course, and the kids he worked with picked their favorite as shorthand. Maybe one of the boys whose stories I’ve mentioned couldn’t remember at all, and paperwork or an interested family member supplied a name different from the one he used every day. Or maybe there was somebody else named Bill, or Stan, on one of those wards, and that someone was unusually protective of his name.
 I probably won’t ever know. Not that particular detail, so specific, and so likely inconsequential, no matter how much I want to read into it. I’ll keep gathering stories, the ones about Stan and the ones about Bill, and I’ll figure out the truth, if not about the name, then about the things that happened, and I’ll line them up for you: in the proper order, and with proper annotation, and with as little of the conjecture I’m making right now as possible. But the writing of this book is about more than just that, and that’s one of the things I’ve been grappling with over the last few weeks, writing and thinking such personal things.
I probably won’t ever know. Not that particular detail, so specific, and so likely inconsequential, no matter how much I want to read into it. I’ll keep gathering stories, the ones about Stan and the ones about Bill, and I’ll figure out the truth, if not about the name, then about the things that happened, and I’ll line them up for you: in the proper order, and with proper annotation, and with as little of the conjecture I’m making right now as possible. But the writing of this book is about more than just that, and that’s one of the things I’ve been grappling with over the last few weeks, writing and thinking such personal things.
I have no idea where I heard this story (yet another damning piece of evidence against my bibliographic skills, which before I started this project left very much to be desired), but it bears repeating anyway. Whether this is a yarn about a real place or an urban legend, a kind of artist’s parable, I don’t know, but it goes like this: there was once a little bookstore with only two sections. Over one cluster of shelves hung a sign that read Facts—nonfiction. And over the other? Truth. The fiction section.
When I first heard that little tale, fiction was the only thing I wrote—at least, the only thing I wrote of my own volition, and the only writing I shared with others that didn’t come back with a letter grade attached. I loved the story then, and I love it still, but it sounds different to me, after all these years, because my situation is different now. I write both. And I think about that anecdote now, and I wonder: why choose just one?
There are things in my novel that reference actual reality, but I didn’t put them there because I wanted anyone to learn anything. Fiction sits on the side of truth, at least when it’s doing its job as it should, and no one asks from it anything more than that—which is exactly as it ought to be. But nonfiction, that’s a different animal. There’s an implied derision in that simple word: facts. It conjures a sterility we remember from textbooks, and it’s a legitimate criticism: I am deeply buried in facts, trying to wade through the existing literature on the history of polio, and it can be stifling. I love to read the scientific papers of the time, which have a sort of sly elegance and cleverness the modern journals I studied in college totally lack, but the secondary sources, the academic tomes, are dry and impersonal in a way that feels to me almost heart-wrenching.
It’s important to provide accurate reportage, and a worthy accounting of the truth. But I love this story because it’s about people. People, and their lives and hearts and minds. People’s families, people’s memories, people’s heritage and hopes. Writers of nonfiction shy from those things, too often. Hoping, perhaps, that people will be able to extract the appropriate feelings from an endlessly unspooling reel of names, dates, and featureless interactions, or perhaps just afraid of accusations of bias or inaccuracy. But that’s the one thing the little bookstore parable has right: facts aren’t, intrinsically, connected to truth. The people I’m writing about deserve better than to be reduced to sweeping generalizations and gut-wrenchingly vague statistics. And they also deserve for someone to tell their stories correctly.
That’s why I look for those signatures, on Bill Stanley Willis William Bell’s letters, and why I pore so carefully over the accounts of those he worked with. Because I think that facts can tell us the truth, if we understand that there’s more there to speak than mere procedure. I love the way the whole world talks to itself: the way the specificity of these anecdotes becomes, always, universal, and the way semantic details can reveal intimate and tender emotions. It’s curiosity about people that leads me to recognize the gaps in my factual, biographical knowledge. It’s because I want explanations for the events and quotations and little quirks of behavior that allowed this thing, this crazy improbability that was the Kenny Institute, to happen the way that it did. And the discoveries I’ve made that way are what convinces me that even good math can add up to something greater than the sum of its parts.
That this story is so emotionally clear and so factually opaque is both its glory and its misery, and I’ve been sledgehammered by that a dozen times since I’ve gotten to Minneapolis. The folders and folders and folders of misfiled letters and papers shuffled like cards in a poker shoe over at the Historical Society are heart-stoppingly overwhelming, and the photographs and jokey newsletters written by Kenny’s patients feel like coming up for air. But I fight through the one to shore up the other. Because—like I’ve said before—I want people to see this thing the way that I do, and I know that means giving you something to latch onto that makes sense. Something that’s real. Something that’s true.
However you choose to interpret that, and whatever name it goes by.
18 Tuesday Jun 2013
Posted in Present Day, Real Life
Tags
introduction, me, minneapolis, moving, present day, real life
Firstly: I owe you an apology.
It’s been almost three weeks since I’ve posted anything, and I didn’t mean to take so much time off from updating the blog. This site is a vehicle for many things—cheif among them educating people about my topic, and keeping them up on the progress of the project—and I’ve been delinquent in both of those arenas. Because there are things I haven’t told you, because I haven’t had a chance. Because I was yanked from something I thought I understood into something that became much more than I bargained for.
It hasn’t been an arbitrary silence, however sudden it might have been. But it was a quiet that fell without warning, I know. (It feels especially egregious to me to have left you all hanging in the wake of my emphatic, anthemic last post.) What to me has been three weeks more chaotic than any in recent memory has been three weeks of radio silence for you. A blank space, a mystery. A vanishing act. And, at least right now, at the beginning of this post, only I know where I’ve reappeared.
The story I’m telling is all about perspective. And so, for the moment, is mine.
A little less than three weeks ago—three weeks that feels like forever, a miniature lifetime not quite my own—I packed up my apartment in Chicago, and watched the past I knew vanish into two dozen cardboard cartons. I’d been considering a move since February, but it wasn’t finalized until April, and nothing felt real until it was happening all at once. Until the internet access clicked off, and the counters had been wiped down for the third time, and the keys were just lying there, on the table where I used to toss the mail.
 Three weeks ago, give or take, I threw my stuff into a U-Haul, and I came here. To this quiet house on a near-silent street, where on Sunday evenings no one breathes, and the sound of fingers on laptop keys bounces noisy off brand-new hardwood floors. A huge blackboard hangs on the wall, blank, for now, but raw with possibility, and on the floor a lamp beams out pale, softly colored light. It’s a grownup house, far more so than any I’ve lived in before, thoughtful in the way it’s put together, and the atmospheric statement it makes. I’m the one who made it that way, over three or four whirlwind days of trips to Target and IKEA furniture assembly, but there’s still something sort of bewildering about it. Something fragile and unreal.
Three weeks ago, give or take, I threw my stuff into a U-Haul, and I came here. To this quiet house on a near-silent street, where on Sunday evenings no one breathes, and the sound of fingers on laptop keys bounces noisy off brand-new hardwood floors. A huge blackboard hangs on the wall, blank, for now, but raw with possibility, and on the floor a lamp beams out pale, softly colored light. It’s a grownup house, far more so than any I’ve lived in before, thoughtful in the way it’s put together, and the atmospheric statement it makes. I’m the one who made it that way, over three or four whirlwind days of trips to Target and IKEA furniture assembly, but there’s still something sort of bewildering about it. Something fragile and unreal.
I live in Minneapolis now: a cozy two-bedroom on the outskirts of a neighborhood called Uptown, a few blocks away from Lake Calhoun. And the transition, which I thought would go so smooth and seamlessly, has changed me in ways I never could have imagined.
 It feels strange to take any part of the story I’m telling for my own, and to feel connected to it so strongly in the present, but it’s been very much on my mind in these last weeks. What it means to be sidelined by something unexpected, and to vanish from a world you share with others into a different one, a smaller one, where you find yourself both more and less alone. A world that can be terrifying, in the possibilities that bloom when you least expect them, when a path you thought was modest and well-defined branches out to dozens of possible successes and failures.
It feels strange to take any part of the story I’m telling for my own, and to feel connected to it so strongly in the present, but it’s been very much on my mind in these last weeks. What it means to be sidelined by something unexpected, and to vanish from a world you share with others into a different one, a smaller one, where you find yourself both more and less alone. A world that can be terrifying, in the possibilities that bloom when you least expect them, when a path you thought was modest and well-defined branches out to dozens of possible successes and failures.
Only so much of any intensely personal journey can be shared. There are limitations on words, ones I grapple with every day, in trying to illustrate the stories of people whose heads I will never entirely inhabit. (Nor is this challenge confined just to the problems of history; though I haven’t talked about it here, I’m also a fiction writer, working on a novel in tandem with this book.) I haven’t even defined them all for myself, the things that have changed since I came here, and that makes the seismic shifts even more difficult to articulate.
But I can say this, and easily enough: even with an overstuffed U-Haul, and all the things I brought with me, I left even more behind.
I came here to be closer to my research. To take the next step in teasing out the truth of the saga I’ve promised to recount, and get a better idea of how to go about the writing process itself. My apartment is a twenty-minute drive from the Historical Society in St. Paul, where they keep those archival boxes I’m always talking about, the ones that spill out stories like a thousand points of light. The site of the original Kenny Institute, the building stripped of its façade (and its purpose), but still recognizably connected to the one in the photo at the top of this page, is a ten-minute drive from my apartment. If there are more people to interview, they are most likely here, or at least their descendants are; my new friend Russell lives in a nearby suburb. The modern Sister Kenny Rehabilitation Institute is (or was, but more on that later) still operating in the Twin Cities, and how much they might be able to tell me of what I want to know remains to be seen.
I knew I was coming here for a reason. But I didn’t realize it wasn’t any of the ones I’ve listed. I didn’t realize that what I’d find in this new home was something I never knew I was looking for, in the midst of a landscape almost entirely divorced from the map I followed to get here.
The first time I ever came to Minneapolis—this city itself, not its wayward brother St. Paul, where I spent research weekends two blustery Januaries in a row—was the middle of this last April. It was the trip on which I found the place I live, when after a long day of frustration and disappointment I stepped into my new living room and asked, “Where do I sign?” But the trip wasn’t supposed to focus on the hunt for an apartment, which, even with my lease in Chicago rapidly running down, felt more like a lark than anything else. I was here for something on the surface very different, but equally dear to my heart: a yoga teaching seminar with the brilliant Matthew Sanford, whose work I’ve admired ever since I found out about it last year.
I got my yoga teacher training certification about a year ago, at the fitness-focused studio where I practiced in Chicago; it seemed like a good opportunity, and a good next step for something that had become incredibly important in my life. I have always lived amidst deafening noise, struggling with anxiety and a chronic lack of confidence, and learning to breathe through yoga infused both my personal and creative lives with new energy, new hope. It was an arena where I thought I might find a deeper connection between myself, and the things inside my head, and other people, and the outside world, all spaces segregated inside me by improbably high walls. But before long I realized I didn’t have the time in my life, or any real longing in my heart, to teach conventional yoga. Leading the Spandex-clad denizens of Wrigleyville through asanas—the fancy word for poses—meant mostly to tone a part of their body with a similar name, was not the personal development I needed.
Matthew Sanford sometimes teaches yoga to people who wear Spandex, and care how they look from the rear. (I know because I’m one of them.) But he also teaches “nontraditional” yoga to people with disabilities—trying to bring to their lives not just the traditional benefits of yoga (mindfulness, calm, self-reflection, and, yes, fitness) but also something else, something bigger. A sense of their bodies as intrinsically whole, and intrinsically valuable, still beautifully connected to and conversant with their minds, whatever their practical limitations or neurological sensations might be. And he does it all from the wheelchair he’s lived in since he was thirteen, his world transformed instantaneously by a car accident.
 The world inside my head softens, when someone speaks directly to my heart. Just reading about Matt’s work melted me, and I knew right away that that was what I wanted to be involved with. The practical challenge of figuring out how to adapt the essence of poses without losing what they try to tell us about the way we exist in the world (“teach the experience,” as Matt puts it), and the subtler challenge of really being with someone as you go through that together. The challenge of real presence.
The world inside my head softens, when someone speaks directly to my heart. Just reading about Matt’s work melted me, and I knew right away that that was what I wanted to be involved with. The practical challenge of figuring out how to adapt the essence of poses without losing what they try to tell us about the way we exist in the world (“teach the experience,” as Matt puts it), and the subtler challenge of really being with someone as you go through that together. The challenge of real presence.
I took his first training session, like I said, in April, and then the follow-up, second-level program in May. What happened inside those light-filled rooms was amazing to me, and unlike so much else in life it existed with all the superfluity stripped away. This is real, Matt kept telling us—the teacher trainees, and his students, too. This is real life.
And I thought, yeah.
Because it’s the same way I feel about this project, and my novel, too, and the parts of my personal life that I hold the most dear. It speaks to the same impulse as the concept of art, and the sanctity of language—which, for me, is just the most convenient stand-in for the idea of honest communication in general. To put one’s hands on a yoga student, or to sit with someone as they confide a transformative story, or write the story of something that never happened, but could have, and share it with someone who understands—that is the closing of a chasm, the bridging of a gap. It is a stretch toward truth by two parties who are both interested in finding it, rather than avoiding it, for fear it might feel uncomfortable.
Matt teaches his adaptive classes at a place called the Courage Center, a facility with both in- and outpatient clients, working to help those with disabilities live more independent lives. And in a partnership that seems to have rocked the local healthcare world significantly, but that I had managed not to hear about until I got here, it was recently absorbed into one of the local hospital systems—the same one that manages the modern Sister Kenny Institute. Neither one will exist any longer independent of the other. And what that meant didn’t hit me until I filed the paperwork to assist in Matt’s class, and got an e-mail back from the volunteer liason at the newly established conglomeration: “Volunteering at Courage Kenny Rehabilitation Institute.”
I came here in part to be near the Institute, which I hear is still doing pretty remarkable work. But I never imagined I’d work there, or in the place that it’s becoming: a place sort of sentimentally near to my heart, which is both new and old and at a crossroads. Kind of like me.
One of the things I love about the Kenny story, and that of the Kenny Institute specifically, is the sense of cohesion it provided for the people who lived there. The hospital’s philosophy gave the patients a framework for understanding the world and their place in it, and whether and how what had happened meant that had to change. It gave them a way to weld everything together, to take a blast furnace of confusion and frustration and anger and put it to work. And that insistence on wholeness of body and soul, on not just picking up the pieces but taking the time to fit them together into a life that made sense, was everything.

I write about wholeness a lot, and spend a lot of time reflecting on it, but it’s something I’ve never really had. The welded life I love so much is one I’ve never lived. The things that I loved, and the different aspects of the person I wanted to be, and the concerns that I always thought were important, never had a chance to manifest all at once. I could do a handful of things at the same time, and if something crucial was missing, I would go looking for it when something else changed, or I found more time, or things weren’t quite as difficult. When I was less anxious about how people might see me, or what they might think, if my carefully curated worlds collided.
But it isn’t true. The realization came suddenly, and hard, in this new living room: that the day when things are easier, or I have more time, or fewer preoccupations, is never going to come. There are a million moments of right now in a lifetime, each one different, and weighted down with context. But right now is the only thing that there will ever be.
I was eighteen years old when I moved to Chicago. I knew a lot about what, and who, and where, I didn’t want to be. (An Apple computer salesperson, stuck in the suburbs of Baltimore, four years out of college and without any idea where to go, or whether I might ever fit in.) But I never felt truly empowered to choose something different. I never found a community where I could be myself, or people with whom I felt compelled to get seriously involved. I yearned for independence: the feeling of independence, of agency, which is far more ephemeral than people realize. I lived on my own for years without ever feeling empowered to drive my own life in the direction I felt it was really meant to go.

I spent a long time shy and embarrassed about my writing, about my past, my philosophy, my life. I still haven’t talked very much about my background, but I’m planning to; I want you to know me, and why I’m doing this, as well as you come to know the people who populate the sepia picture I’m painting. I don’t want to write myself into my own book; the end product this blog teases is about Elizabeth Kenny, and the people she helped (and some of those she couldn’t), not about me. But talking about the process is inevitably a way of talking about myself, especially now that my thousand shattered lives are sharpening, finally, to a single point.
I lived a yoga life, before. A life as a fiction writer, and a separate life as someone embarking on a research project that seemed impossibly audacious, given my background: an undergrad degree in biology didn’t seem legitimate enough to speak on such a momentous topic, and my five years in the pediatric ER of Johns Hopkins Hospital felt like an inadequate explanation of my interest in medicine. I never talked about my writing with strangers. I’ve lived lives in secret, and lives that were highly visible but not quite true. I’ve never spent much time trying to fit into others’ expectations, but I have spent long years being wistfully misinterpreted by the people around me. I have tried silence, and I have tried angry, self-righteous defiance, but I have never tried acceptance. I have never stood still in the midst of myself and acknowledged the things about me that are unchangeably true, or honestly tried to escape the traps I fell into by accident, and than stayed in out of fear and inertia, the ones filled up with easy, painful lies.

What does it mean to embrace being lost, when it takes even more bravery to admit to being found? There is no agreed-upon scorecard in life, at least not one any useful number of people will agree on; you will never know if you’ve “won.” The only judge worth listening to is the barely audible voice inside your head, whispering breathily that you’ve done the right thing, and it’s all too easy not to listen. Because what if you’re wrong? What if it’s made-up, and this thing seems so wonderfully laden with potential just because it happens to be better than the terrible situation you’d been mired in before? What if you are merely the victim of a fresh landscape, and the wishful thinking that comes along with it?
What if it doesn’t matter? Who the hell cares? Wishful thinking is a cynic’s synonym for hope. Perception is reality. And we write our own stories every minute we’re alive.
Everything is different here. The weather is different: unseasonably cool and sticky, and unremittingly gray (unusually, the locals promise), with a ceiling of clouds that peel like wallpaper. The people are different: they move more slowly than I’m used to, and talk more sharply, about places and things whose names I don’t know. The neighborhood is another world, with its quiet residential streets and quilted flower gardens, sitting apart from the vintage shops and bike vendors and dive bars on Lyndale. There are as many restaurants in my entire neighborhood as there were in the five blocks around my old place. Even more of the twentysomething hipsters stalking down the streets sport slashes of neon color in their short-cut hair, but they look more out of place than they did in Chicago. More ostentatious, but quietly so, circumscribed in their defiance.
I am different here, but not because of any of that. Because when everything you know falls away, your first instinct is to do everything in your power to find those things again, and snatch them back, keep them safe. And the liberation in realizing that maybe they aren’t the ones you need after all—that is beautiful, and terrifying. And something it’s going to take a lot longer than three weeks to sort out.
My journey is far less dramatic than that of the kids that I write about. I have not been blindsided, traumatized, or terrorized (at least not in the short term); if my world has been upended, it has been by something that at least on the surface I chose. But that doesn’t mean I know exactly where I am, or have a good grasp on where I’m going, or that keeping the faith is always—or ever—simple. It’s a positive change, this one that I find myself so unexpectedly facing, but it is one I feel unprepared to handle, even as I hope to use it as a springboard to the kind of wonder I’ve never successfully held. I’m hoping I can learn from them—Kenny’s kids, the ones that I feel I’m watching over, now, in this place with so many memories, and so many echoes of beauty. With fortitude, and a little bit of luck, I’m here not just to tell their story, but to follow their example.
I am definitely still a little lost here. But sometimes, when you’re lucky, in being lost to the world, you get a chance to find yourself.

28 Tuesday May 2013
Posted in Introduction, Kenny Institute, Society
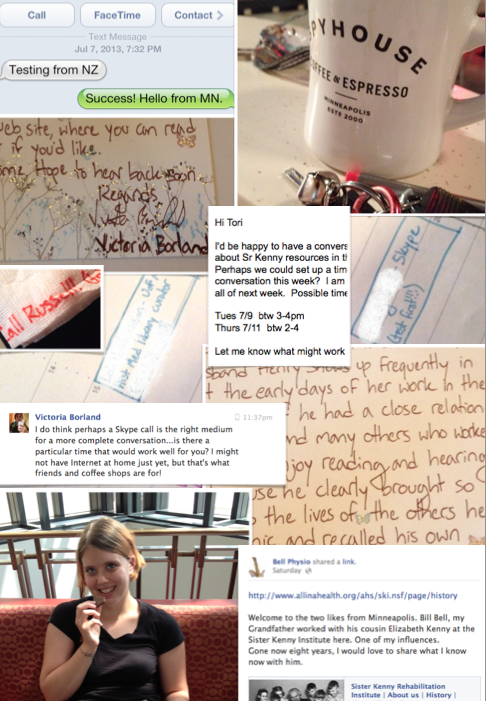
There is a lot of amazing stuff, in the stack of ludicrously heavy filing boxes that make up the Minnesota Historical Society’s “Kenny Papers.” But one of the more arresting parts of the collection is a thick folder of letters, newer than most of the things housed there, and without their musty smell and air of fragility.
Some of the letters are written by hand, in the beautiful looping calligraphy kids don’t learn anymore; I certainly couldn’t replicate those effortless, soaring curves. Others are tapped on typewriters, or printed in erratic monospace font, spat out unceremoniously by early word processors. They come on paper of every imaginable color and size, some intricately folded, others not at all. There are short ones, barely a paragraph, and ones that seem to go on forever, and it’s obvious that none of them say anywhere near as much as they could. Some are creased razor-sharp, the lines so straight they seem to have been written across a ruler; others sprawl and squirm, thick paper rippled by moisture, the residue of sweaty hands or falling tears.
I’d swear that even after all this time–exactly as many years as I’ve been alive–some of them still carry a faint whiff of elegant perfume.
They’re letters written about the still-extant Sister Kenny Rehabilitation Institute on its 50th anniversary in 1992, when a prominent Minneapolis newspaper asked former patients to contribute their memories of the time they spent there. And the differences are semantic, because the content of every single one is the same. I’ve never seen the initial request, but it must have been restricted to the very earliest patients, from the forties and very early fifties, the ones who knew Sister Elizabeth Kenny personally. Or maybe they were simply the ones who felt moved to write in en masse.
The letters are incredibly, unreservedly warm, and to a one palpably grateful. These people, fifty years later, remembered their time at the Insitute—or “Kenny,” some of them called it, “my time at Kenny”—with nostalgia almost unto joy. The time they had spent as inpatients in that squat little building in the heart of Minneapolis was time they’d come to treasure. And they wanted, so exuberantly, so delightfully, to tell their stories. To explain how their brimming, happy lives had played out, and thank everyone involved, even though so much time had gone by that most of the Institute’s original staff had passed away.
It’s fantastic. There really isn’t any other word for it. I came to these things after months immersed in the kind of desperate material I spoke at length about in the last few posts, a world drenched in fear and viewed perpetually in the negative: with the deep pessimism of resignation, and in garish, otherworldly colors. I saw none of that here. And what I saw instead enchanted me.
Who in the world was this woman, I wanted to know, and what was so different about this place?
As it turns out…that depends very much on who you ask.
Even though I’ve been researching her story for upwards of a year now, I’m still trying to tease out fact from fiction, and half-truths from the ones so complete they’ve been embellished into legend. It’s one of those stories, the best kind: where the most hyperbolically ridiculous statements are the ones most likely to prove true, and the ordinary things, the ones that establish a simple, everyday rhythm of life, are the toughest to pin down.
The lives of extraordinary people aren’t so different from anyone else’s, day in and day out. But those aren’t the things people remember.
 Born in 1880, Elizabeth Kenny grew up in rural Australia, part of a large, rambunctious family with a formidable number of children. Easily the most fearless and outgoing member of an already free-spirited group, when she broke her arm as a teenager, she convinced the doctor who set the bone to take her on as an apprentice. (Though she would later claim various nursing certifications, this may be the only supervised medical training she ever got.) After a couple of years spent working on and off for Dr. McDonnell, she ventured out on her own to serve as a “bush nurse.” It was somewhere in the depths of these years, making house calls on horseback to families who lived dozens of miles from anything approaching “civilization,” that she started treating polio cases.
Born in 1880, Elizabeth Kenny grew up in rural Australia, part of a large, rambunctious family with a formidable number of children. Easily the most fearless and outgoing member of an already free-spirited group, when she broke her arm as a teenager, she convinced the doctor who set the bone to take her on as an apprentice. (Though she would later claim various nursing certifications, this may be the only supervised medical training she ever got.) After a couple of years spent working on and off for Dr. McDonnell, she ventured out on her own to serve as a “bush nurse.” It was somewhere in the depths of these years, making house calls on horseback to families who lived dozens of miles from anything approaching “civilization,” that she started treating polio cases.
The story of her very first encounter with the disease is a great one, and I won’t tell it here, at least not right now. But the crux of the story is contained in a single telegram sent by Kenny’s mentor, after the young, terrified nurse reached out for help.
“Infantile paralysis,” Dr. McDonnell told her. “No known cure. Do the best you can with the symptoms presenting themselves.”
And so Kenny did—and her young charge made a full recovery, along with the half-dozen others who fell ill in the outbreak. She had no idea what you were “supposed” to do with polio patients, or even what was assumed to be wrong with them. It’s a big leap, actually, from “this patient can’t move so well” to “this patient is paralyzed,” and in circumventing the conventional wisdom—not because she was rebelling against it, but because she didn’t know what it was—Kenny found loopholes and inconsistencies in that thinking that led her to an entirely different method of treatment. Among other things, gentle exercise took the place of immobilization, and intense heat therapy stood in for bizarre drug injections—and the results were spectacular. (I am being, here, intentionally vague; a further explanation of these competing treatments, and the way Kenny’s approaches to neurology and psychology intertwined, is in the pipeline.)
With a couple of brief detours into other endeavors, Kenny worked from that point forward rehabilitating people with disabilities who had been written off as hopeless—not just polio patients, but also kids with cerebral palsy and other neuromuscular disorders. As word of her method (and its effectiveness) spread, so did the controversy: she claimed to observe dramatically different symptoms than had been recorded by anyone else, the symptoms on which her method was based, and an air of self-righteous indignation started to gather around her.
One of my very favorite lines in her (spectacularly funny, and spectacularly fictionalized) first autobiography, published in 1943, tells you pretty much everything you need to know about her manner of interacting with others: “Some minds,” she says, “remain open long enough for the truth not only to enter but to pass on through by way of a ready exit without pausing anywhere along the route.”
This was not a clever aphorism devised to get a smile out of readers. It was a philosophy by which she lived, and if she thought you suffered that particular affliction, she was not shy about telling you so. A contemporary journalist might have called her the “Angel of the Outback,” but Elizabeth Kenny was hardly a saint. (Nor was she a nun, despite being widely known as “Sister” Kenny; that was a title bestowed upon decorated nurses in the Australian army, where she served during the First World War.)
 Part of the reason I decided to do this project is the frequency with which people still try to discredit Kenny, on the rare occasions when the story is dragged out of the historical attic, and that modern prejudice is rooted in the ferocity of the original controversy. Doctors loathed her, almost to a one, because everything about her rankled—her gender, her lack of credentials, the fact that she said they were wrong—and when they rebuffed her, she pushed back with equal ferocity. She was right, obviously, and everybody else was not only wrong but also incredibly stupid. (This is a diplomatic strategy that tends not to further negotiations.)
Part of the reason I decided to do this project is the frequency with which people still try to discredit Kenny, on the rare occasions when the story is dragged out of the historical attic, and that modern prejudice is rooted in the ferocity of the original controversy. Doctors loathed her, almost to a one, because everything about her rankled—her gender, her lack of credentials, the fact that she said they were wrong—and when they rebuffed her, she pushed back with equal ferocity. She was right, obviously, and everybody else was not only wrong but also incredibly stupid. (This is a diplomatic strategy that tends not to further negotiations.)
It wasn’t until 1940 that she landed in the United States, and there’s some confusion about why she ended up here in the first place. To hear her tell it, she was sent by the Australian government and its public health counsel to spread her technique as a point of pride for her country; less generous accounts sometimes imply that they wanted very badly to get rid of her. But after unsuccessful presentations at hospitals in New York and Chicago, just as she was about to return to Australia, she met a duo of sympathetic doctors from the University of Minnesota hospital…and it was in Minneapolis that the other side of the story blossomed.
Kenny might have been combative with doctors (and, when necessary, politicians, the press, and her own staff). But to her patients, she really was something like a saint. Gentle and attentive, she was their constant defender from a system that didn’t take them any more seriously than it took her. They became co-conspirators, in a way, and it was an arrangement that seemed to strengthen everyone involved. Kenny didn’t have time for anybody’s—well, it’s not exactly a family-friendly word. But she always had time for her kids.
Russell Papenhausen, the gentleman I interviewed a few weeks back, who I’ve mentioned a couple of times, lights up when he talks about her. At age fourteen, he was one of her first patients in Minneapolis, treated before the Kenny Institute (her very own 80-bed hospital, founded in 1942) even existed. And he put it more simply, and with more authority, than any of my pretty words ever could.
“She was a marvelous woman,” he told me, breaking into a mischievous smile. “She put the fear of Christ in the grownups and nothing but love in the youngsters.”
 This was the one time that the patients’ voices won out, and, almost overnight, the beleaguered nation fell in love. Everyone in a position of prominence during the height of the polio epidemics gathered around them many dozens of sycophants; Basil O’Connor, the (extremely reluctant) director of the March of Dimes, was lionized by many, chief among them President Roosevelt. But not many people had letters sent to them asking, in all seriousness, “Would you let me know when it would be practical for you to receive a 15 lb. ham?”
This was the one time that the patients’ voices won out, and, almost overnight, the beleaguered nation fell in love. Everyone in a position of prominence during the height of the polio epidemics gathered around them many dozens of sycophants; Basil O’Connor, the (extremely reluctant) director of the March of Dimes, was lionized by many, chief among them President Roosevelt. But not many people had letters sent to them asking, in all seriousness, “Would you let me know when it would be practical for you to receive a 15 lb. ham?”
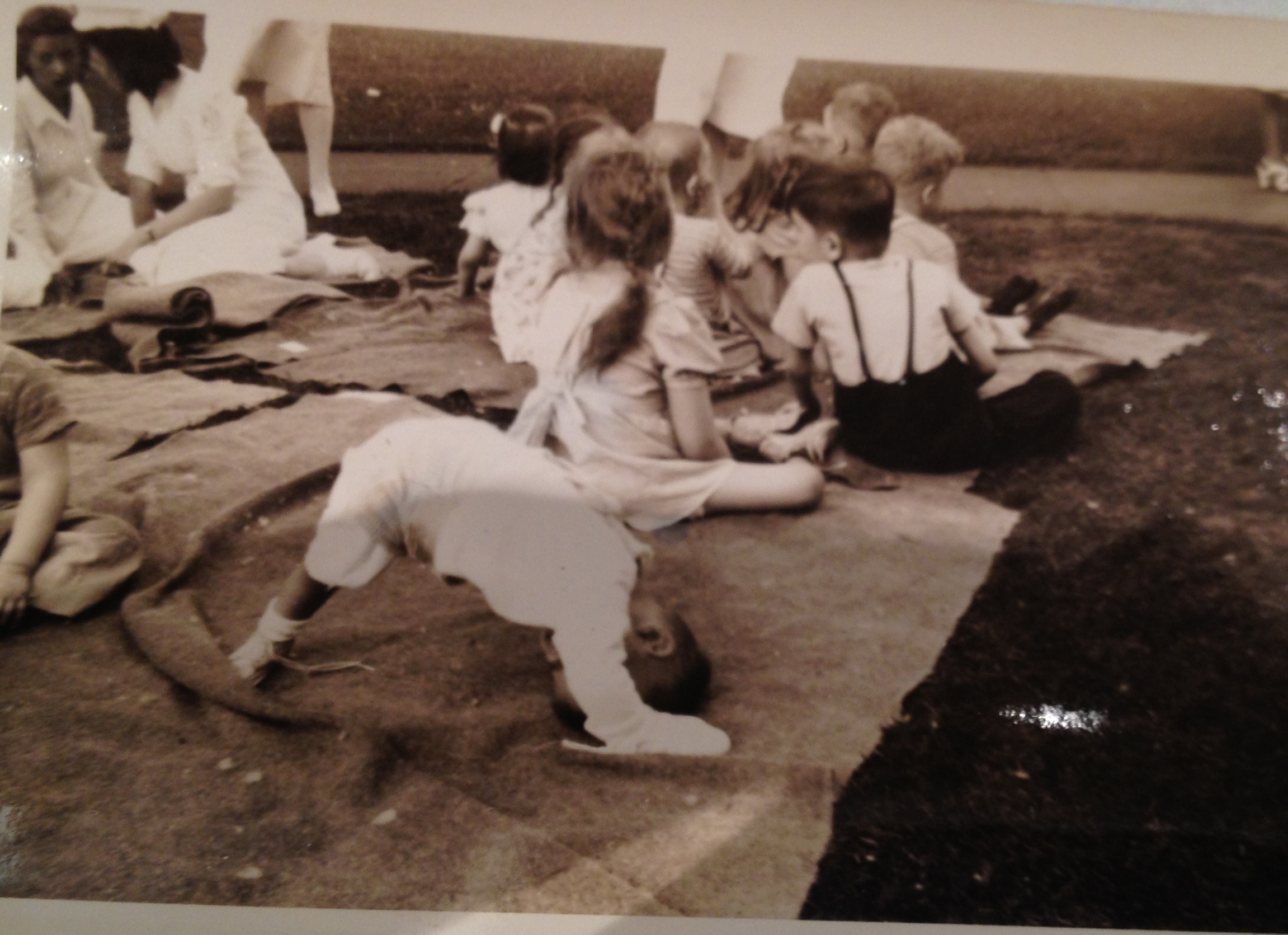
A reporter named Inez Robb wrote the following, after her first visit to the Institute, with the breathless lack of objectivity endemic to midcentury journalism:
When I went out to the institute, I went up to visit a patient in the big ward which houses 29 boys ranging in age from 6 to 16. When I came into the ward, I saw a sight that stopped me in my tracks. Two lively kids of seven were wrestling vigorously in a hospital bed. It was a rough and tumble scrap.
At that moment, the nurse reappeared.
“Tommy! Johnny!” she said authoritatively. “Stop that at once! Tommy, you know you are not allowed out of bed. Get back into your own this instant!”
The kids looked sheepish. Tommy, a beguiling imp with big black eyes, got back into his own bed.
“Kids have so much pep,” the nurse said. Kids with infantile paralysis with pep! With too much pep!
“It seems like a miracle,” I said helplessly.
Kenny hated the word miracle—because it embarrassed her, she always claimed, and because it wasn’t true; I suspect it had more to do with the fact that it gave God credit she would have preferred to keep for herself. But of course it seemed like a miracle. It seemed like a miracle to the uncountable, unfathomable number of parents who had been told their child would never walk again, and to the children who’d believed their lives were forfeit—but for very different reasons. In her baker’s dozen years in America, Kenny tiptoed, and sometimes blithely trampled, the vanishingly thin line between what society expected from a great healer of polio victims and the kind of compassionate care those people actually needed.
Kenny was beloved by the nation for the results she produced: the Kenny Institute’s recovery rate was vastly greater that of any other treatment facility’s—about three times higher than average. More of her kids walked; eventually some ran and jumped and fought for our country in the Second World War (including my new friend Russell). Few wore braces or endured the spinal curvature common among polio survivors; if they used crutches, they were the short forearm type known then as “Kenny sticks,” rather than the awkward underarm variety, the kind you were supposed to use when you broke an ankle, and which gained an extra sense of pathos in their permanence. The science, however controversial, was sound; the therapy worked. Kenny’s kids got better.
But her patients didn’t love her because she made them well. They loved her because—against all odds, in a situation just once removed from the fires of hell—she made them happy.
 I think my favorite thing in the Kenny papers—more touching than the huge box of thank-you letters, more chaotically revealing than the hundreds of disorganized photographs—is a box of newsletters, crudely typewritten sheets the patients at the Institute put out at various intervals in the 40s and early 50s. They were sent out to kids’ families and circulated inside the clinic, blurry duplicates on brightly colored sheets of cardstock, rife with good-natured ribbing and inside jokes. The young writers gossip innocently about their therapists and doctors and nurses, gush about the photography classes they’re taking or the movies brought in for them to watch, speculate about what they’ll do when they get out, who they’ll be when they grow up. They tease with enthusiasm old friends who come back for outpatient visits, especially when their subpar performance in the checkup meant they’d have to come back for a kind of remedial stay.
I think my favorite thing in the Kenny papers—more touching than the huge box of thank-you letters, more chaotically revealing than the hundreds of disorganized photographs—is a box of newsletters, crudely typewritten sheets the patients at the Institute put out at various intervals in the 40s and early 50s. They were sent out to kids’ families and circulated inside the clinic, blurry duplicates on brightly colored sheets of cardstock, rife with good-natured ribbing and inside jokes. The young writers gossip innocently about their therapists and doctors and nurses, gush about the photography classes they’re taking or the movies brought in for them to watch, speculate about what they’ll do when they get out, who they’ll be when they grow up. They tease with enthusiasm old friends who come back for outpatient visits, especially when their subpar performance in the checkup meant they’d have to come back for a kind of remedial stay.
Because, the authors declared, only half joking, they knew nobody ever really wanted to leave.
I find myself holding my breath while I read them, like suspending the present can take me back in time, or like if I wait long enough or attend closely enough I might be able to inhale the stale air, with its sweetly rancid scent of rambunctious kids at play. There’s plenty of irony in the Kenny Stretch, and more than a little dark humor, but hardly anywhere do you see a forced smile. Isn’t this such a weird, messed-up world we live in? they ask, unselfconscious, and wise beyond their years. Isn’t this awful? Aren’t we bizarre?
Yes. And gloriously so. Because their lives belonged to them, and them alone, and it’s clearer here than anywhere else. Nobody else got to decide how they felt, or what they were afraid of. They might have been far from home, stranded apart from everything they knew or understood, but this new world was one they were building themselves.
The Kenny Institute was no less of a microcosm than any other inpatient facility—more so, actually, with its tight restrictions on visitors, and conspiratorial sense of community—but it wasn’t a place where you waited for your life to start up again. It was a place where you celebrated the life you still had, the one you were living, because someday was far away, and you were still exuberantly breathing right now. Though she never stated it explicitly herself, it’s obvious that it wasn’t just Kenny’s therapeutic concept that differed from the norm. Her philosophy was wildly different, too, and its core postulate was this: that recovery wouldn’t happen unless you were deeply invested in it yourself, and that in order to be willing to sink such physical and emotional effort into an outcome that was ultimately so uncertain, you needed to value yourself right now.
Her patients had to understand what they were working for, and that that work was something they did for themselves. Not for some anonymous coalition of doctors who poked and prodded at your limbs and scribbled down incomprehensible numbers on a chart, who wouldn’t tell you if you failed. Not for parents who worried that a lingering disability meant giving up on everything they’d hoped for you in life—not to mention what the neighbors would say, or how the checkbook would balance. Not to keep up with siblings or friends or an amorphous notion of what it meant to have dignity.
And—perhaps most importantly—not even because Sister Kenny told you to. Sister Kenny was not afraid of telling you to, and in no uncertain terms, but—unlike pretty much everyone else in the rehab community, at least according to the patients whose accounts I’ve read—she wouldn’t make you do much of anything at all. If you couldn’t prioritize your own recovery, couldn’t take the initiative to focus on getting better—which meant deciding that getting better mattered, which in an uncertain world must have meant you mattered, at least enough to try—she knew she couldn’t force you to succeed, any more than those stubborn doctors could force her to shut up.
You couldn’t just choose to get better.
But you could choose to live.
Put even more simply: “back to normal” wasn’t under your control, or, however skilled her hands and gilded her reputation, Sister Kenny’s. Recovery depended on factors no doctor or therapist could possibly foresee, on the degree of stripping in the wires, on the strength and stubbornness of your body. But better—partly in the sense of performing “better,” to whatever degree you accomplished that, but also partly in the sense of feeling better, feeling safer, more whole—that was a choice. And it was one you had to make; no one one else could make it for you.
That kind of responsibility was terrifying, especially to kids coming out of hospitals where they’d been treated as all but inanimate. But it taught them to stand up straight—in more ways than one—without feeling like they were being puppeteered. Not everybody remembers the Kenny Institute as a wonderful place to be, and it wasn’t an unconditional blessing for anyone. The reality of this situation was impossible to ignore—even if it was, eventually, possible to escape—and patients were asked to face it head-on far more often under Sister Kenny’s care than at most other facilities. The physical and psychological demands she placed on children widely believed to be both incredibly fragile and uselessly damaged were enormous. But those expectations were also an endorsement of personhood, and a gesture of respect, and for even the youngest of her patients, those confidences were transformative.
“You were lucky,” Russell’s wife told him, at the end of our second interview, after we’d fallen silent, exhausted, companionably sharing a plate of homemade cookies she’d brought.
He looked up, quizzical, in the middle of a bite.
“Not lucky to have polio,” Andree amended, waving a hand. “But lucky she came along when you did.”
It was exactly the same sentiment expressed by the wire-service reporter I quoted earlier, in a different, later piece: the children of Minneapolis, at that particular juncture of history, were the “luckiest in the world.”
Not because they were safe; nobody in the world was that, in the midforties, from polio or anything else. Not because there was nothing horrifying about their world, or because that world was free from danger. Because they had the thing that we all so desperately need, and that so much of the rest of the country at that point lacked.
They had hope. And more than hope, they had agency: the courage to find their own voice, and the fortitude to know that the only way to keep their illness from defining them was to write that definition themselves, before anyone else had a chance.
 This is the story I’m telling. And this is “A Louder Silence”: the embrace of volume, and clamorous voice, in the midst of a world determined to strip away all the noise. The chattering static of undisguised reality, and the way it starts to sound like music, if you tilt your head just exactly the right way. And the other kind of silence, lurking underneath such fearless self-expression: the ability to sit quietly inside yourself, to find some kind of peace, without needing to thrash away at endless, anxious insecurities. To shout with joy, rather than defiance.
This is the story I’m telling. And this is “A Louder Silence”: the embrace of volume, and clamorous voice, in the midst of a world determined to strip away all the noise. The chattering static of undisguised reality, and the way it starts to sound like music, if you tilt your head just exactly the right way. And the other kind of silence, lurking underneath such fearless self-expression: the ability to sit quietly inside yourself, to find some kind of peace, without needing to thrash away at endless, anxious insecurities. To shout with joy, rather than defiance.
Of course, it’s not always that easy. It’s probably never as easy as I just made it sound. But it was possible. It was beautiful. And this silence deserves to be amplified.
Welcome home.
25 Saturday May 2013
Posted in Introduction, Society
She is grim and anxious, captured in this set of black-and-white photographs. Her small body rigid, she stands barely balanced on a pair of short forearm crutches, mouth set and sharp as a razor blade. You can see how much she needs this step, and how hard her heart must be beating, keeping time with the shaking of her weak, tangled muscles as she moves. Her therapist’s hands are light on her slender legs, her ankles and calves, moving them forward one at a time, showing her where to go, making the effort she is still too wrung out to manage by herself. Her short hair is neatly braided, pretty and incongruously ordinary against the back of her neck. She’s maybe eight years old, or a little older than that, and she looks exhausted already, holding the weight of the world in her small hands, eyes fixed straight ahead.
And then something changes. I don’t know what happened in that moment, in the flicker of time between those shutter flashes (if shutters, or flashes, were even things cameras had back then). I wish I could have been there, to see exactly what elapsed between the fourth and fifth snapshots. But whatever it was—some whispered word of encouragement, or some feeling of triumphant familiarity—looking at that last picture is like watching the sun come up. Standing there, laughing, she is radiant on those crutches, this skinny grade-school girl. Elfriede Kohler is the happiest person in the world.
The day I saw that picture was the day I started to understand. What I was really looking at, and what someday I would be writing about, and what it would come to mean, and the ways that it would change me. Those photographs are the culmination of a lengthy scrapbook, lovingly assembled by someone at the clinic where Elfriede was treated, chronicling her progress from the depths of illness to partial recovery and discharge. The brown kraft paper is rippled and torn, and pictures have fallen out here and there, leaving tantalizing holes in the story that the handwritten captions don’t quite manage to fill.
And I sat there in the library, feeling the weight of this book in my lap, as fragile and enduring as the girl it preserves, and I knew I never wanted to give it back. Not just because the feelings were so profound. Because—at least in part—I was starting to grasp just how incredibly rare they were.
Moments like Elfriede’s don’t come along very often, in these stories, but even when they do, they sit far down the line from the place we left off. The illness was a dark, purgatorial space, after the before but just before the after, and no matter who you were, and what you might eventually achieve, the earliest forays into this new, unstable life were as terrible as anything that preceded them.
Polio’s paralysis is strange and unpredictable: its boundaries are fuzzy, its consequences vague, and, at least at the beginning, its permanence unclear. Weakness powerful enough to put someone in an iron lung could abate entirely within weeks, but someone else’s comparatively inconsequential limp might never get better at all. The effects are hardly ever symmetrical, nor are they especially well-contained: one side of the body is almost always much more heavily involved than the other, and even devastated limbs usually have some muscles that still work.
Even more uncannily, for all the glittering pins and needles of the illness itself, once the infection clears, sensation is rarely ever affected. So much of the world stays intact: the feel of the damp sheets against your body, the nurses’ rough handling of your tight, aching shoulders, the bright-lit pain that still pulses through your body, random and blinding as lens flare. It’s only your ability to interact with it that changes.
It doesn’t make sense, the straining that happens inside you, and the cruel disconnect between what you feel or imagine to be possible, and what you find really is. Some people talk about a sense of disembodiment, like that part they can still sense but can no longer command or comprehend doesn’t even belong to them anymore. More often, though, in recounting their experiences, people don’t talk about it at all. They are lying desperately ill in the contagion ward, and then they are in therapy, transferred somewhere else to reboot, to get better. The transition is so fast and so disorienting, and the things on either side of it so bold, that it doesn’t even stand out.
Every so often, someone will bring it up, often a little dreamily, like they’re only just realizing it’s true: I guess that was the last time I walked on my own.
Knowing seems to bring them comfort.
It was clear right away that something was terribly, terribly wrong, but it often took a long time to figure out just what it was. The moment it was possible to endure being touched again, the doctors swarmed back in—more often than not to contain you, compress together all your pain and confusion and complicated feelings and literally bind them to your body. Not just weeks but months of recovery were spent lying strapped down in bed, in an attempt to prevent further damage to weakened muscles. Infants were put into body casts; older children and adults found themselves racked on “Bradford frames,” traction-like devices that held them stretched out, often with their arms at right angles.
“The immobilization is maintained for a period of eight weeks, a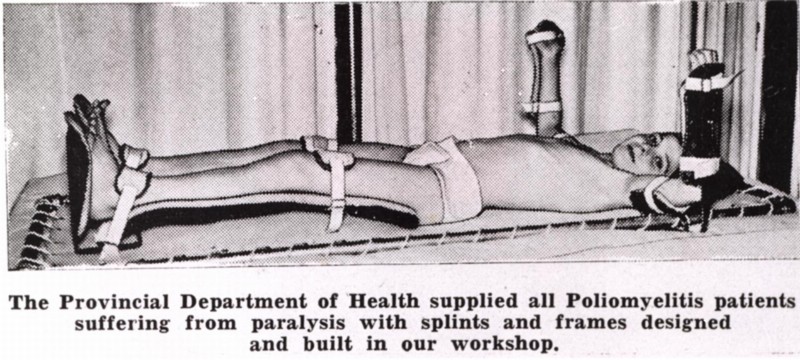 t which time a second muscle test is made…. If exceptional improvement is shown, this immobilization…is repeated,” a prominent 1941 textbook, Dr. Philip Lewin’s Infantile Paralysis, instructed. These eight-week periods were to be repeated indefinitely, but were “seldom continued for more than six to eight months.”
t which time a second muscle test is made…. If exceptional improvement is shown, this immobilization…is repeated,” a prominent 1941 textbook, Dr. Philip Lewin’s Infantile Paralysis, instructed. These eight-week periods were to be repeated indefinitely, but were “seldom continued for more than six to eight months.”
As if that’s no time at all. As if everyone old enough to understand what was happening to them didn’t use that time to think about what would become of them after all this was over. Didn’t lie in bed worried and helpless, and knowing all too well what would happen if it didn’t work. If they didn’t get better.
People don’t talk about the transition, and those early days and weeks of recovery. But they talk about the extremes to which they later went to fight for normalcy. They talk about being haunted by a stigma they were desperately trying to avoid.

There’s a poster that’s frequently reprinted in historical retrospectives of the “polio years;” I first saw it in a 2005 exhibition at the Smithsonian Museum of American History in Washington D.C. Created for a vaccination awareness campaign in 1956—the second summer the shot was available—it shows two different pictures, dramatically-split screened by contrasting backgrounds. On the right stands a smiling grade-school girl in tight buns that bear a passing resemblance to Princess Leia’s, balanced awkwardly on wooden crutches, the angle of her slender arms calibrated to imply even more deformity than she seems to suffer. On the left, two able-bodied children stride confidently through a field, wholesome hands intertwined.
This, the caption reads, above the happy siblings. Not this, above the bravely grinning girl. Vaccinate your family now
This. Not this. This. Not this.
This was the world the many thousands of people paralyzed annually by the disease in the U.S. alone had to live in.
Every single depiction of polio, every warning against it, characterizes the disease as a hideous specter, sometimes literally so: in a film called The Crippler, produced by the March of Dimes, the illness moonlights as a grossly elongated shadow, looming darkly over unsuspecting homes. Polio was horrifying, of course, and more than likely this visceral repulsion accomplished its objective: eliciting donations, raising awareness, and getting kids vaccinated, when that time came. But in associating the illness with the grotesque, its victims were tainted that way, too. As disgusting and contaminated, or else tragic and courageous, almost martyred, helpless young sacrifices to a noble cause. We put these kids up on pedestals even as we shrank from them in terror.
Having polio no more made you brave than it made you broken. It meant you were in the wrong place at the wrong time, that you shared the wrong ice cream cone or dove in the wrong swimming pool. The poster child was a cultural fantasy, not a reflection of reality.
But how do you understand that, at four years old, or fourteen? You’d seen those pictures, unless you’d been living under a rock since the day you were born. You knew what it meant, to have had this happen to you. And you knew that the only way to be okay again, to avoid being pitied or lionized, was to get better. All the way better. Even the kids in those posters knew it: “Help me walk again,” a picture of a child in a walker pled, and a happily skipping boy was triumphantly captioned, “Your dimes did this!”
Getting better became the only thing that mattered. The only way to feel real again. And not just getting better. Getting well.
In the mem oir Warm Springs, about her surgical rehabilitation at FDR’s famous polio hospital, Susan Richards Shreve recalls her younger brother asking if going in for reconstructive operations frightened her.
oir Warm Springs, about her surgical rehabilitation at FDR’s famous polio hospital, Susan Richards Shreve recalls her younger brother asking if going in for reconstructive operations frightened her.
“I’m not scared,” she told him. “The next time you see me, I’m going to be a different girl.”
“What kind of girl?” he asked her.
“A perfect one.”
It wasn’t just the specter of posters in shop windows and hyperbolic movie reels that made this seem so crucial. It was the reality you lived, day in and day out, in most inpatient rehab facilities. After the restraints finally came off, patients were often started on aggressive exercise regimes, hoping to strengthen them enough to get them back on their feet. The goal, always, was sitting, standing, walking, no matter how much supportive bracing that required, or how much it might hurt.
 The acceleration was dizzyingly brutal: kept from doing anything for so long, now you were expected to do everything, and the goal wasn’t really to make you feel better. It was to achieve something as close to normalcy as possible, no matter how strenuously your weakened body protested, and when inevitably you ran up against something you really couldn’t do, it felt like your fault. Like you’d failed somehow.
The acceleration was dizzyingly brutal: kept from doing anything for so long, now you were expected to do everything, and the goal wasn’t really to make you feel better. It was to achieve something as close to normalcy as possible, no matter how strenuously your weakened body protested, and when inevitably you ran up against something you really couldn’t do, it felt like your fault. Like you’d failed somehow.
And once those insurmountable roadblocks were found, the limits of your natural recovery defined—at least as far as the (misguided, but we’ll get to that) doctors were concerned—the next step certainly wasn’t acceptance. At a time when fighting to win at any cost—not just in the battle against polio, but in nearly every circumstance, great or small—was not only virtuous but expected, acceptance felt synonymous with giving up. Encouraging someone to come to terms with their disability was unthinkable: if the patients didn’t feel adequately distressed about how they were doing, what reason would they have to keep struggling?
The next step, instead, was surgery. Surgery to fuse bones, to transplant tendons from functional muscles to paralyzed ones, to shave down joints unhinged by muscle cramps. Dozens of surgeries, sometimes, stretched out over years, trying to account for growth, and the pernicious influence of time. For the most part, these procedures were designed not to make the patient feel more comfortable, but to make her more conventionally functional, closer to “normal”—whether or not that was something she actually wanted, or that her weakened body could support.
Lest you think I’m being hyperbolic, or exaggerating the extent to which recovery alone restored legitimacy, I want to share some excerpts from a March of Dimes pamphlet meant to “help” affected teenagers cope with the aftermath of their illness. There’s no date that I saw on this slender, seemingly innocuous document, but I’d bet anything it came from the mid-40s, with both fear and determination at their most histrionic peak.
“Everyone has problems to solve. Some are easy. Some are hard,” it begins, with an understatment that feels almost deadpan. “When you are ill your problems are more difficult to solve, more annoying, and many times you do not know where to turn for help.”
Then the language turns from merely patronizing to aggressively fraught with expectation: “it is…the function of the National Foundation to help you win your way back to health.” You and your family are “fighting to defeat the effects of the polio virus insofar as human skill and knowledge can do so”—and human skill and knowledge were held in high esteem at the time, with the country deep in the throes of new American exceptionalism, awestruck by unfathomable advances like the atomic bomb.
“If this little book does help you to ‘learn the score,’” the introduction concludes, “if it helps you become better able to conquer your polio and return to a full and happy life, it will have done everything we hoped it would do.”
There is no space, in that tone of enforced cheerfulness (which continues, blithely, through the rest of the booklet), for anyone whose recovery is less than triumphant. There are only winners and losers, without space left to to carve out a life in between—when life in between was most often the reality you confronted. No doctor ever asked a child when enough was enough, or how she felt about what was happening to her. They certainly never asked the darkest, and perhaps most crucial, question: Do you even want to get better?

It seems like an absurd thing to ask, doesn’t it? Of course you’d want to get better. There was nothing redeeming, hardly even anything tolerable, about this illegitimized existence, lost in the darkness of constant discomfort, at the mercy of a system you didn’t understand. But what the doctors failed to understand was this: rehab felt like a kind of limbo, a probationary period, where the rules and privileges of normal life were suspended. It was the place where you stayed while you waited to find out if your sentence would be commuted, and as long as you were there, everything else seemed far away. More often than not, the “real world” these kids were supposed to be fighting to rejoin seemed like nothing but a cruelly impossible dream.
It’s hard to convince yourself to work toward a goal with such a narrow definition. A difficult but attainable challenge is motivating. But it’s hard to imagine enduring that sense of futility, day in and day out. Lying in bed able to move just an arm, or a couple of toes, knowing that walking, that better, that normal, was the goal, made every incremental victory along the way seem less a triumph than an unbearable reminder of you how far you had to go.
Even if they couldn’t articulate it, there had to be some part of them that understood the paradox in which they were now unwillingly complicit. If you couldn’t get better, phyiscally speaking, but you had to get better, in order to win back your legitimacy as a human being, your right to take up the same space and breathe the same air as other people without inspiring revulsion or reverence, then what were you supposed to do? There had to be something you could do.
And there absolutely was: you could deny it.
Not that it had happened; that would have been absurd, not to mention impossible, for someone in a wheelchair, or encased in a body brace. But you could refuse to acknowledge that it had affected you. You might be in the chair, but the chair wasn’t a part of you. You were normal. It was your disobedient body that was the problem, and that didn’t really need to have anything to do with you. This whole thing was merely a formality, some kind of terrible joke, and you would reenter the world determined to prove that the real you was better than this chair you sat in.
At the end of the day, in order to be seen “just as yourself,” people felt forced to deny a huge, and hugely formative, part of who they had become. What had happened didn’t fit into anyone’s plan, or anyone’s image of what they wanted for themselves. But to refuse to alter that image at all, and to make a perpetual enemy of the crutches that held you up or the fingers that drifted uselessly at your side, created problems all its own. Insisting that you were unaffected, unchanged, un-limited, was an understandable reaction, but it was also a profoundly disingenuous one. Whether it came of the work ethic instilled in therapy, or developed as a defense mechanism to cope with the world thereafter, relentlessly having something to prove drove polio survivors to be—statistically!—much more accomplished than their healthy compatriots. But it also delayed, and in some cases denied, their ability to find peace.
I’m not implying that anyone failed, or that what anyone did was wrong: these attitudes were adaptive. Patients developed the skills they needed to live in a world that felt hostile and warped, out of line with all of their possible realities. They believed what their doctors and nurses and parents told them, and what kids don’t? What person doesn’t, under sufficient duress, cling to anything said with enough confidence and certainty? They needed a way out of the terrible place bad luck had landed them, and that way was better. At any cost. Better was a solid, straightforward goal. And that was comforting.
But there was another way.
It’s hard to give up that one clear goal, with its easy answers about who you are supposed to be and what you ought to want, and embrace uncertainty instead. It’s hard to accept things as they are, and keep picking your way across the river one rock at a time, turning with the currents of the water, neither frozen motionless in terror nor so desperate to push forward that the rapids sweep you in and pull you under. Rushing through the process was as impossible, and trying as disastrous, as lying back passively and giving up. It wasn’t just your “wholehearted cooperation and obedience when working with the physical therapist” (and doctors, nurses, and parents—again, according to the booklet) that made the difference. It was your ability to cooperate with yourself, and thereby learn to navigate the actual reality you lived in, rather than the one other people said you did.
It’s why I love that picture of Elfriede so much. What shines out through her eyes isn’t relief, or hope for the future, visions of what might come next. She isn’t dreaming of barefoot running or high school dances, or even setting down the crutches to stand on her own. She’s just happy. She’s found her feet again, and it feels amazing, and as far as she is concerned—she, and her grinning therapist, who seems equally delighted—in that moment that is enough. At that moment it’s everything.
That feeling—and the fact that it’s possible—is as rare and precious as her smile. The human spirit is astonishing, and it’s no surprise that some managed to evade the limitations pressed upon them, and navigate these labyrinthine preconceptions to make their way on strength of spirit—and an enduring sense of self—rather than pure force of will. There are plenty of beautiful stories scattered across the smooth, impassive surface of this seemingly unscalable edifice. But nowhere do they cluster as tightly as they do around Elizabeth Kenny—the nurse I mentioned in my first post, the one this book I’m writing is about—and the Minneapolis clinic she presided over for twelve years.
It’s not Kenny, in the pictures of Elfriede, which were taken somewhere on the outskirts of Germany, sometime in the early 1940s. But the young woman whose touch pulls the little girl forward into her moment of heart-stopping joy was a Kenny-trained therapist. And I’ve seen enough to know that what this mysterious revolutionary imparted to her charges—the therapists she taught, and the patients she treated—was as much philosophy as technique. And it came at a time when we all sorely needed a paradigm shift.
I’m looking forward to showing you around.
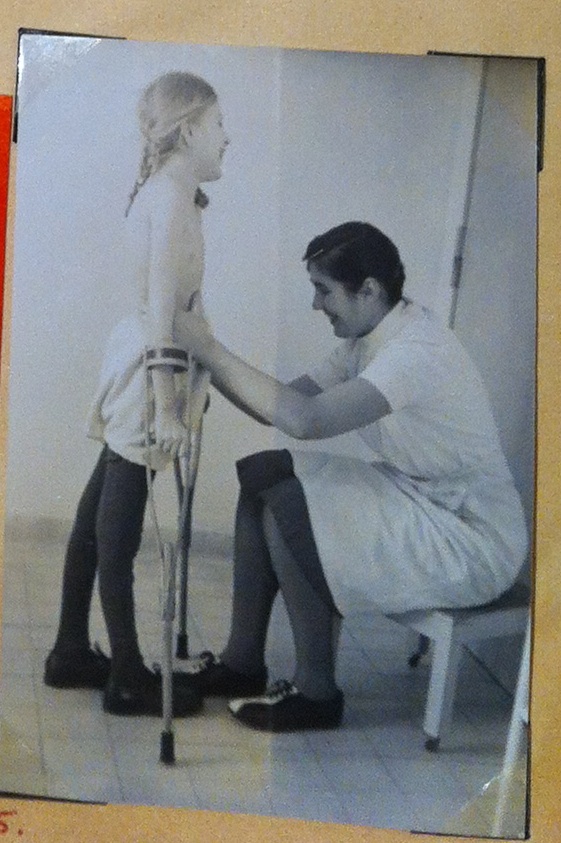
13 Monday May 2013
Posted in Introduction
Tags
What scares you more: the thing you don’t see coming, or the one you can’t escape?
I guess you can learn a lot about a person from how they answer that question. I’ve been staring at it for days, and I don’t know if I could tell you where I fall—especially if we’re asking not as a horror movie audition, where that verdict is the end of the story either way, but as something both subtler and more awful, where the choice is only its beginning.
Polio isn’t loud, at least not at first, not the way I think we wanted it to be. The way people must have imagined it was, in a world constantly haunted by propaganda that managed to feel defeatist even as it pledged to do the conquering. The March of Dimes—which I realize I’ve mentioned several times without any real explanation, but trust me, before long you’ll know more than you ever hoped for—waged a ferocious war against it for twenty long years, drafting a huge swath of the nation’s mothers into the fight, and when you go into battle, you like to imagine you know the enemy. You want something ugly to point at, to hate, something as obviously repulsive as the villainous offenses themselves.
In the end, the brutal truth of polio is that the answer to the question doesn’t matter. It didn’t differentiate, one way or the other; more often than not, its victims confronted both. The metal temples to its sinister domination, the iron lungs and braces like birdcages, became the symbols we raged against. But the reality of the experience itself was often a much quieter, sadder undermining—and hardly anyone ever knew when to steel for the impact.
It was an ordinary day. Or it was an extraordinary one, but you remember it as ordinary, eerily so, in the same way that, when you ask someone to tell you about a landmark catastrophe, something like September 11th, they so often talk first about the weather. It was such a beautiful day.
A day marked not with searing agony or sudden weakness—not usually, at any rate—but with something more insidious: a missed step, a stubbed toe. A late-spring school day spent with your head on your desk, the sound of your classmates’ pencils on test papers suddenly unbearable, your own exam still untouched in front of you. A blank space in a conversation, a sudden gaping where there should have been easy words.
 Your stomach hurt. Your head hurt even more. Trembling chills canceled out the summer sun, and your throat was so sore it hurt to talk. Those first few days were miserable, in a way I think we’ve all endured at one time or another: thoughts furred with fever, aching all over, too tired to move except during sleepless nights spent running back and forth to the bathroom. Icky. Exhausting. But not the stuff of brimstone nightmares.
Your stomach hurt. Your head hurt even more. Trembling chills canceled out the summer sun, and your throat was so sore it hurt to talk. Those first few days were miserable, in a way I think we’ve all endured at one time or another: thoughts furred with fever, aching all over, too tired to move except during sleepless nights spent running back and forth to the bathroom. Icky. Exhausting. But not the stuff of brimstone nightmares.
For all the hype about polio, unless you lived in the midst of a raging epidemic, at first the possibility occurred to almost no one. The same mothers who forced children to touch chin to chest every time they came home from the playground, checking for the hallmark neck stiffness, sent their sick kids to bed with nothing but a couple of aspirin, and maybe a hot-water bottle to soothe slender, aching limbs. Maybe it was self-defense. Maybe it was just ignorance—ignorance to the real threat, subsumed by its distorted public image. In the anxiety-ridden, war-torn first half of the twentieth century, you quite literally had to pick your battles, and every single tummy ache couldn’t trigger a full-on lockdown.
But however innocuous it looked on the surface, from the very beginning something was different. There’s no one thing people can point to, asked to recall exactly why they felt so awful, but even in its early stages polio was something to be suffered, rather than merely waited out. Everything about it threw the world off-balance: the overwhelming nausea, the disproportionate vertigo that made the ground seem to sway, the pricking pins and needles turning touch to sandpaper—intermittently now, and, as the illness progressed, in great drenching waves of skin-crawling sensation.
Children wept. Adults wept, too, sometimes, or else they turned tense and irritable, hypervigilant with anxiety. It’s possible the emotional sensitivity came of the viral scouting parties already mapping out territory in the brain, or it could have been something else; we probably won’t ever know for sure. But the disease was such a profound misery that medical manuals often listed “inconsolable” behavior as a genuine symptom, one that contributed significantly to the likelihood of a positive diagnosis.
Sometimes it got better. Sometimes the fever broke, and stability returned, the nagging sense of the world viewed through a warped pane of glass dissipating overnight. For the most part, those people never knew there had been anything so seriously wrong with them at all. Never knew just how close they’d been to the kind of precipice that dissolves beneath your feet. They blamed bad food at a barbeque, or that night they went to bed with hair still wet. And then they carried on with their lives, the lucky ones.
But maybe you weren’t so lucky. Maybe the headache that had merely nagged for days turned blinding, molten metal pouring down the nape of your neck until your whole spine was stiff as iron. Maybe you hadn’t been able to keep anything down all weekend, and suddenly found you couldn’t even swallow the water in the glass you so unsteadily held. Maybe the soreness in your calves, a strain that used to feel just like adolescent growing pains, turned overnight to cramps so bad they made you cry.
And the parent or partner to whom you’d confessed darted off to call the doctor, and left you to sit with the spark of terror you’d watched kindle in their eyes.
This was the moment of truth: the collision of your world with the hellish one you heard on the radio and saw in movie-theatre public service announcements, the one the media constructed to evoke pity and fear in equal measure. There were so many things you should have suspected, but didn’t, precautions you ought to have taken, signs you should have seen. Adrenaline made your stomach drop, this time, rather than nausea: what was going to happen now, if it was true? Had you gotten somebody else sick? What would become of your brothers and sisters, your parents, your kids?
What would become of you?
With very few exceptions, the doctor took one look—at the ginger way you held your body, how you winced at bright light, the limp as you walked or the unnaturally exaggerated curve of your spine—and sent you straight to the ER.
 There you were met with either an overwhelming rush of activity or a long and interminable wait. During an epidemic, lines stretched for hours, and only those already struggling for breath were allowed to skip ahead; if you had the misfortune of being the first case in town that season, the entire establishment descended on you in one predatory blink. One way or the other, a single detail was constant: the forceful violation of the spinal tap, a single point of anguish to slice through the broad blur of misery. Confirming a diagnosis required a sample of spinal fluid, collected by curling a victim already painfully rigid into a fetal position, and then sliding a thick needle between two vertebrae until clear liquid trickled out.
There you were met with either an overwhelming rush of activity or a long and interminable wait. During an epidemic, lines stretched for hours, and only those already struggling for breath were allowed to skip ahead; if you had the misfortune of being the first case in town that season, the entire establishment descended on you in one predatory blink. One way or the other, a single detail was constant: the forceful violation of the spinal tap, a single point of anguish to slice through the broad blur of misery. Confirming a diagnosis required a sample of spinal fluid, collected by curling a victim already painfully rigid into a fetal position, and then sliding a thick needle between two vertebrae until clear liquid trickled out.
There was no anesthesia for this procedure; frequently there was no explanation for this procedure. You might never have found out why it was necessary. But you never, ever forgot it.
The instant the diagnosis was final, complete isolation began. Children and parents (and husbands and wives) were separated, often by force; neither knew when they might see the other again, or if it might be in a coffin.
So then there was silence, and you were alone.
The fuss of admission and diagnosis gave way to the heavy void of solitary isolation, or the eerie quiet of an open polio ward, filled with the labored breathing of a dozen others just as sick, and the palpable tension of their own unspoken fears. Still nauseous, still disoriented, likely still sore and headachy from the spinal tap, patients suddenly found themselves afflicted with something new: invisibility.
“I didn’t know what the hell was wrong with me,” Russell told me last week, fingers twisting together, gaze cast down to the kitchen table. Russell, my interviewee, who fell ill when he was fourteen, and talks about it like it happened a year ago, instead of seventy-three.
“They didn’t tell you?” I asked, incredulous.
“Oh, they could’ve,” he shrugged, without missing a beat. “But I probably didn’t understand what they were talking about.”
It’s a revealing thing to say: for all the paranoia surrounding the idea of the illness, hardly any of the kids it ensnared had any idea what it would look like if it assaulted them. Neighbors worse off than you were terrify ing, and wardmates in recovery, objects of seething, fevered envy; none of you had any idea what was going on. Doctors dismissed the notion that even adults or teenagers had the right or ability to dictate their own medical care. No one asked you what you wanted, what you needed, how you felt—or if you were okay with any of the many confusing, uncomfortable things they might be doing to you.
ing, and wardmates in recovery, objects of seething, fevered envy; none of you had any idea what was going on. Doctors dismissed the notion that even adults or teenagers had the right or ability to dictate their own medical care. No one asked you what you wanted, what you needed, how you felt—or if you were okay with any of the many confusing, uncomfortable things they might be doing to you.
“I had a temperature of 106 for ten days,” one girl says matter-of-factly, in a book of short interviews called Polio Voices. The brain is supposed to rebel against this sort of thing; the “thermostat” in the hypothalamus has this number set as its absolute upper limit, since at that point the risks start to outweigh the defensive benefits the body gets from running a fever. It’s not necessarily dangerous, intrinsically, but it tells us something about how completely beholden to the virus its victims became, once it infiltrated the nervous system. And once you were in the hospital, you couldn’t just go to the cabinet and pull down a couple of aspirin. You couldn’t get up to walk to the bathroom—either because you were too weak, or because you were under strict orders not to exert yourself. (It was thought—correctly, it seems—that any activity after the onset of spinal infection would worsen the ensuing paralysis.)
 Things crop up in these stories over and over again that would be horrifying if they happened just once. The repetition gives them a kind of melancholy sadness, a strange, dark wonderment at the workings of this microcosmic world: just a cursory skim through the reminiscences in the books I’ve collected turned up three people who had overheard someone saying that they’d died. To lie there in the dark, unable to wrestle away a sheet pulled up too high, lightheaded, breathing so shallowly the doctors apparently didn’t notice—the patients knew they were alive. Maybe. But everything about the illness was so surreal it’s hard to believe they were sure.
Things crop up in these stories over and over again that would be horrifying if they happened just once. The repetition gives them a kind of melancholy sadness, a strange, dark wonderment at the workings of this microcosmic world: just a cursory skim through the reminiscences in the books I’ve collected turned up three people who had overheard someone saying that they’d died. To lie there in the dark, unable to wrestle away a sheet pulled up too high, lightheaded, breathing so shallowly the doctors apparently didn’t notice—the patients knew they were alive. Maybe. But everything about the illness was so surreal it’s hard to believe they were sure.
It felt like the world was ending, every illusion of comfort and safety shattered in a single sledgehammer blow, and you had nothing to do but sit at the window watching shards of clinging glass drip down one by one, and wonder what manner of demon would climb through the gap next. And that dark inner world felt impossibly strange, pressed up against the bustling, well-lit one you lived in, where doctors hurried from one bed to the next saying words even adults didn’t understand, and except in the most horrible extremity the nurse showed up at the same times every day to give you juice and take your temperature. The whole universe had gone mad, but except for the occasional shrieking outbursts of a roommate unable to cope or some poor soul down the hall, it wasn’t a derangement with any external confirmation.
The roiling sea—the riptides of fear, your churning stomach, the uncertainty of rescue and the Kraken lurking always just beneath the waves—was contained entirely inside you. And who were you, so clueless, so sick, so unstable, to say if any of it was even real? The doctors seemed indifferent, when they even noticed or remembered you were there. Your body was betraying you, this shell you’d so thoughtlessly relied on in homeroom and games of kickball, at work and in the bedroom, and so why should you believe the blinding agony it felt? Maybe the problem was just your delirium. Maybe you were the problem. Who was left that you could trust?
So you did your best to stay quiet and composed, to be brave and not make a fuss, while sweat-crusted sheets rubbed your tender body raw. The oceans of salt, at least, those were real: polio brings on drenching sweats—“diaphoresis,” in doctor-speak—out of proportion even to the fever.
And you waited. Floating.
The brain is precious, and the body knows it. Dying nerves—nerves dying, as I said in the last post, stretched and popping like overinflated balloons—don’t go quietly. As the static on the line between the muscles and the brain grows louder, the illness shifts from a vague, squirming discomfort to a fierce and violent possession. Muscle cramps far too powerful to stretch out lasted for days, so persistent that frequently they didn’t relax even after the fever broke. A sensory condition called hyperaesthesia, in which normal sensations feel exaggerated and sometimes painful, made the pressure of the bedsheets so unbearable metal frames were used to keep them from touching patients. Spasms and tremors shivered through burning-hot bodies, sometimes confined to an unsteady hand, other times triggering whole-body shocks like the ones that sometimes happen as you’re drifting off to sleep.
Leaving you at the mercy of a torturer you could neither see nor explain. There was no wound to point at, no captor to loathe. No amount of struggle made it any better; mental effort was exhausting, and most physical treatments just made the pain worse. In many ways, this is far more terrifying than the notion of a sudden, sweeping paralysis: a body’s refusal to cooperate is scary—and sometimes infuriating—but not nearly as much so as being betrayed by it, backstabbed so primitively by something you couldn’t escape.
 The specter of mortality was unrelenting, with silent bodies carried out through rooms still quietly full of life, and dire prognoses issued loudly at bedsides, as if their occupants were already too far gone to hear. The constant humming wheeze of the iron lungs carried with it a very particular ambiguity: for a child feeling breathless in the dark—fatigued by dehydration, weak with creeping spinal infection—just the sight of the machine was a tremendous relief. But if you went into that hulking contraption, would you ever come out again? Most people did, after a few days or weeks of rest, letting the pressurized chamber do the work that tired breathing muscles couldn’t. But some would stay there for the rest of their lives. And lying there, growing weaker by the hour, exhausted and sometimes delirious, how could you possibly think about anything else?
The specter of mortality was unrelenting, with silent bodies carried out through rooms still quietly full of life, and dire prognoses issued loudly at bedsides, as if their occupants were already too far gone to hear. The constant humming wheeze of the iron lungs carried with it a very particular ambiguity: for a child feeling breathless in the dark—fatigued by dehydration, weak with creeping spinal infection—just the sight of the machine was a tremendous relief. But if you went into that hulking contraption, would you ever come out again? Most people did, after a few days or weeks of rest, letting the pressurized chamber do the work that tired breathing muscles couldn’t. But some would stay there for the rest of their lives. And lying there, growing weaker by the hour, exhausted and sometimes delirious, how could you possibly think about anything else?
The iron lung was the most famous intervention, but it was hardly the only one—and in many ways it was the least extreme. Something called “convalescent serum” was crafted from the blood of polio survivors, on the premise that their antibodies would bolster the response of the immune system currently under assault. Curare, an extremely potent poison, causes paralysis with a rapidity the poliovirus can only envy; the sick were sometimes put on ventilators and injected with the toxin, in case total motionlessness could slow the viral spread. Vitamin injections irritated overtaxed bodies, and often did more harm than good.
 All that’s just the medicine, though; the physical regimen was equally dramatic. Some patients were immobilized in splints to keep them still, restrained like the mental patients they might have begun to empathize with, while shuddering involuntary movements swept through their bodies. Others were bundled into steaming wool compresses and wrapped in rubber sheeting to relax their spastic muscles; this was one of the only effective interventions, but it must have been hard to believe it was doing any good, when the fever was so high they had to alternate heat therapy with rubdowns of ice. The single most lifesaving revelation in the treatment of bulbar—brainstem—polio was the practice of tilting patients’ beds so their heads were inclined towards the ground, lower than the rest of their bodies. Not because this made it any easier to breathe (that role, for those patients, was played by “rocking” beds, whose mechanized swing back and forth coerced the diaphragm into something like a normal pattern of expansion and contraction). Because those patients often lacked the reflex power to swallow their own saliva, and letting it drain down their chins kept them from fatally choking.
All that’s just the medicine, though; the physical regimen was equally dramatic. Some patients were immobilized in splints to keep them still, restrained like the mental patients they might have begun to empathize with, while shuddering involuntary movements swept through their bodies. Others were bundled into steaming wool compresses and wrapped in rubber sheeting to relax their spastic muscles; this was one of the only effective interventions, but it must have been hard to believe it was doing any good, when the fever was so high they had to alternate heat therapy with rubdowns of ice. The single most lifesaving revelation in the treatment of bulbar—brainstem—polio was the practice of tilting patients’ beds so their heads were inclined towards the ground, lower than the rest of their bodies. Not because this made it any easier to breathe (that role, for those patients, was played by “rocking” beds, whose mechanized swing back and forth coerced the diaphragm into something like a normal pattern of expansion and contraction). Because those patients often lacked the reflex power to swallow their own saliva, and letting it drain down their chins kept them from fatally choking.
 In this firestorm of painful detail, I’ve lost the thread of the story I was telling. Misplaced that anonymous person on that curiously beautiful day, the one sent so unceremoniously out to sea. And maybe I’m making excuses for my own labyrinthine writing, my struggle to wring coherence out of this huge and elusive topic, but it feels appropriate, somehow. All this skipping around is fitting: losing threads and finding them again, later, when the context has changed, and they seem to mean something else. Being in this situation was a constant exercise in triangulation, struggling to figure out where you were—mentally, medically, spatially—and what the hell that meant. Losing yourself, over and over again, and repeatedly rediscovering a person not quite the same as the one you’d left behind.
In this firestorm of painful detail, I’ve lost the thread of the story I was telling. Misplaced that anonymous person on that curiously beautiful day, the one sent so unceremoniously out to sea. And maybe I’m making excuses for my own labyrinthine writing, my struggle to wring coherence out of this huge and elusive topic, but it feels appropriate, somehow. All this skipping around is fitting: losing threads and finding them again, later, when the context has changed, and they seem to mean something else. Being in this situation was a constant exercise in triangulation, struggling to figure out where you were—mentally, medically, spatially—and what the hell that meant. Losing yourself, over and over again, and repeatedly rediscovering a person not quite the same as the one you’d left behind.
That was the person you’d have to carry back into the world with you, when all this was over. Being sick with polio was awful. But the acute illness was a thing with boundaries, a fever dream with a beginning and an end. You woke up one day—a week into the trial, or maybe two or three—with sheets even more thoroughly soaked through than usual, and the sun was a little brighter, and your head a little clearer. Gravity had tripled, and your body felt sore and reluctant, in the places that it worked at all. The fever had broken, and a line had been crossed. For some the moment came as a tremendous relief; for others, that first self-check felt more like a sentence handed down after a long, squeamish deliberation. Maybe you’d be sent home, after a few weeks of recuperation, or maybe you’d be entering the scary, uncertain world of inpatient rehabilitation, but either way, one thing was true. You no longer had polio. You were a survivor.
And that was a thing that you never woke up from.
01 Wednesday May 2013
Posted in Present Day
Tags
So that last post I made was very carefully engineered to have a follow-up within forty-eight hours or so…and then I spent the last forty-eight hours coordinating a hugely exciting interview instead, and driving halfway across the country to conduct it.
It’s tomorrow. I can’t wait.
The cliffhanger might stick a little longer than anticipated. But I’m still here. Still working. And hopefully I’ll have some big stuff to share very soon.

29 Monday Apr 2013
Posted in Introduction, Science
Tags
Let me say this straight out: polio is not an easy thing to write about. Not an easy thing to characterize, anyway, without distorting it, without allowing some kind of bias to creep in. And in saying that, I join a long tradition of skewed perspective: it is impossible to paint a clear-cut picture of polio because such a thing doesn’t exist. Sixty or seventy years ago, a thousand questions went just barely unspoken in millions of households across the country: how dangerous was the disease, really? How likely was it to disable you permanently if you caught it? Who was most vulnerable—rich, poor, black, white, girl, boy? How many communities would it strike? Would it strike me, here, today?

If knowledge is power, they were grasping at straws. In some years there were 20,000 diagnosed cases; in others, three times that. Sometimes an individual outbreak paralyzed only one in a hundred victims; other times, one in two. Adults were more likely to end up devastated, but children caught the disease in greater numbers. Cancer killed many more people each year than polio, but polio did cause 22% of all physical disabilities among New York City’s children in 1944, and most of the other causes were congenital, inborn. Epidemics began like clockwork in mid-June, rumbled inexorably toward August, and faded to murmurs by late September, and we still aren’t entirely sure why.
If you believed the March of Dimes’ alarmist public service announcements, and took the tragic, lovely poster children who smiled from shop windows to heart, you were probably too terrified to ever leave your house. Affronted doctors worked constantly to counter newspaper coverage that reported casualties in offset boxes like sports scores, tired of calming parents who believed a diagnosis presaged certain death, and if you believed them you probably weren’t worried enough. The approach modern commentators tend to take runs something along the lines of, “Well, the public probably percieved polio as a greater threat than it actually was, both because it was so frightening, and because the media coverage of it was so extensive.” Which is true. But it’s nothing like a conclusion, nothing like information, nothing like clarity.
If the story of polio is anything, it’s a tale about the ways in which perception transforms into reality.
But it’s also science, of course, and science is objective and explainable—at least, we like to think it is. The world is unpredictable, and things we like to think of as absolute are too often contingent on variables beyond our control. There are so many different presentations of the virus, so many possible “clinical syndromes,” that an early medical text proposed eight or nine different “types” of polio-related illness; all were drastically distinct, and at least half potentially fatal.
This, at least, is true: polio is caused by a virus, the uncreatively named “poliovirus,” part of the same family as the viruses that cause most stomach upsets and a half-dozen different kinds of common cold. The word itself is a little bit bizarre: squat, and kind of ugly, and if you don’t know its Greek root, meaningless. A shortened form of poliomyelitis, I’m not sure knowing what it means makes things a whole lot better: polios is Greek for “gray,” and a myelitis is inflammation of the sheaths that protect the nerves of the brain and spinal cord. And they did mean “gray brain swelling” literally: it was merely a blunt description of the damage done to the nervous systems of those who died from the disease. Their nerve tissue would be drained of color on autopsy, faded to grayscale from its normal healthy pink.
The gray death. It doesn’t have quite the same ring to it as bubonic plague, but if you found yourself in its path it was every bit as terrifying.
Viral infections propagate in several ways, but the most common, the one that the poliovirus uses, is especially brutal and crude: once the virus enters one of the body’s cells, it replaces the genetic material that carries the cell’s “instructions” with its own. Rather than producing the proteins that keep us alive and healthy, the cell begins to churn out endless copies of the virus. Unlike the proteins, these new viruses have no way to escape the cell, and the membrane swells until it bursts. Too devastated to repair itself, the cell dies, and uncountable new viruses flood the surrounding tissues, looking for new cells to colonize, so the cycle can begin again. (There is a particularly good illustration of this the National Museum of American History web site.)
When this happens in the initial stage of the infection, when the invasion is “systemic”—distributed throughout the body, replicating mainly in the stomach—this is unpleasant, but not especially devastating. The vast majority of the body is more than capable of regenerating, after the immune system kicks into gear, and a few long days of misery come to an end. It’s when the infection burrows deeper that the stereotypical paralysis occurs: once it breaches the nervous system, the poliovirus has a particular, peculiar affinity for the nerve cells known as the “anterior horn cells” of the spinal cord. These cells form the chain reaching from the brain, where the impulse to move originates, down the spine to the muscles, where the contraction itself occurs. And with each cellular “lysis,” those connections grow weaker and weaker, until the line finally, agonizingly, goes dead.

We move more than we realize. As I’ve been sitting here, I’ve readjusted in my chair a half-dozen times, crossing and uncrossing my legs, boosting myself up to tuck them underneath me. When I’m at a loss for words, I crack my knuckles, wiggle my toes, push my hair obsessively behind my ears and then ruffle it free again. During one particular stuck moment I got up for a quick set of jumping jacks. Even typing requires a spectacular coordination, and when I think too hard about how it happens my fingers stumble on the keys. It’s almost surreal to think that these things we do so thoughtlessly, these incredible fluid movements, originate as nothing more than electric shocks, racing through our bodies at literal lightning speed. But that’s exactly what they do.
Muscles are dumb. I’ll talk far more about them later, when I discuss physical therapy in more detail, but they just aren’t terribly ambitious: the only thing an individual muscle fiber knows how to do is contract. It doesn’t even know anything about relaxing, not really: it’s either on, and squeezing, or it isn’t. And somehow these many thousands of binary decisions, distributed throughout the six hundred and fifty muscles that string us together, make possible the incredible feats of dexterity we think nothing of every single day. I could talk about ballet dancers and sculptors and ultramarathon runners. But I prefer to think of the astonishing complexity of small things: cooking breakfast. Writing by hand. Putting on shoes. Getting in and out of chairs. Pushing up on tiptoe to reach that thing on the top shelf.
It’s those things you miss the most when they’re gone.
But I’m getting ahead of myself.
As I alluded earlier, polio is on the most basic level a stomach virus. It’s where the infection usually originates, and it’s where the infection in most cases stays. “Abortive” polio, it’s now called, and it isn’t any fun—the sore throat is wicked and the nausea can be debilitating—but if that’s the extent of the infection, after a couple of days you’d be in the clear. (Most of the time, anyway: in some cases, the symptoms disappear for a few days in a kind of “dormant” period, before returning again with much greater ferocity. Polio narratives are thick with these kinds of frightening uncertainties, and the sense that no one was ever quite entirely safe.)
 The next possible manifestation of the disease, for those not fortunate enough to recover right away, is called simply “nonparalytic polio.” It’s more properly a meningitis, which most people have heard something of: an inflammation of the lining that covers, and under most circumstances protects, the brain and spinal cord. It’s a different kind of infection from the bacterial meningitis that sometimes makes the news, but it’s still extremely uncomfortable and potentially very dangerous. The compression on the nervous system causes extreme sensitivity to light and sound, and dramatic stiffness of the neck and back, with a headache so severe and sudden it’s sometimes described as a “thunderclap.” But as long as the poliovirus stays around the nervous system and not inside it, when the fever breaks and the pain subsides, the exhausted rigidity vanishes with it.
The next possible manifestation of the disease, for those not fortunate enough to recover right away, is called simply “nonparalytic polio.” It’s more properly a meningitis, which most people have heard something of: an inflammation of the lining that covers, and under most circumstances protects, the brain and spinal cord. It’s a different kind of infection from the bacterial meningitis that sometimes makes the news, but it’s still extremely uncomfortable and potentially very dangerous. The compression on the nervous system causes extreme sensitivity to light and sound, and dramatic stiffness of the neck and back, with a headache so severe and sudden it’s sometimes described as a “thunderclap.” But as long as the poliovirus stays around the nervous system and not inside it, when the fever breaks and the pain subsides, the exhausted rigidity vanishes with it.
In anywhere from five to fifty percent of cases—the three different “strains” of the virus varied greatly in severity, as did the accuracy of case reporting—the infection keeps pushing deeper, until it breaches the tender innermost spaces. Stereotypically, the virus spreads through the nervous system in an “ascending paralysis”: entering at or near the base of the spinal cord, the virus climbs that chain of cells, spidering its way back up towards the brain, ravaging the cells it commandeers in the process. The body is wired more or less from the bottom up, too, so that so-called “milder” paralytic infections, choked off quickly by a panicked immune system, leave behind the leg weakness typically associated with the disease.
As the damage rises, the difficulties become more sweeping and severe: about halfway
up the back sitting becomes a struggle. A little higher, and moving the arms is all but impossible. As the infection pushes into the uppermost segment of the spine, the cervical spine that flexes in the neck, breathing is suppressed; that’s the area wired to the diaphragm, which controls the inflation of the lungs, and just above the rib muscles that expand and contract to make room for them.
In what is arguably the most extreme form of the illness, it creeps all the way up to the base of the brain itself (“bulbar polio,” referring to an archaic term for the brainstem), which controls everything we do without thinking about it. It keeps our hearts beating. It keeps us from forgetting to breathe. It sends the signals we need to digest food properly, and governs reflexes like the one we use to swallow it. It controls our body temperature and our sleep. And it can be torn apart as surely as the motor neurons.
The fallout from that, as you can imagine, is devastating.
I tell you these things because it’s important to understand the mechanical assault, to fully grasp the firestorm happening inside patients’ bodies. It’s important to understand because these facts form the basis for the incredibly contentious debate that erupted over the best practices in physical therapy for polio. I tell you because I want you to know what we’re dealing with, and the magnitude of the physiological destruction it wrought.
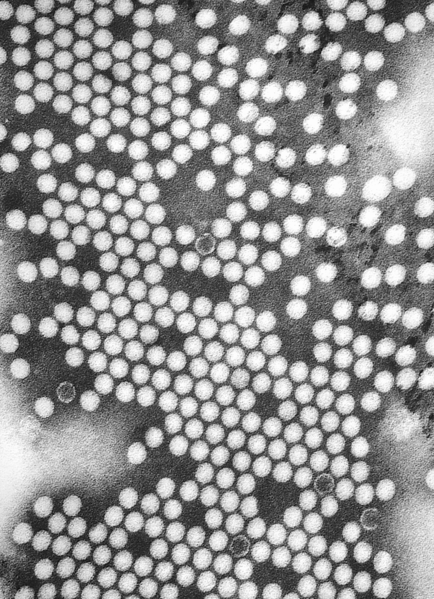 But understand this, too: we didn’t even know most of these things for sure, back in the forties and fifties, when this terror opened up communities like it was ripping out a seam, warping the pattern of everyday life, exposing the fragile, private lining from which we tried so hard to avert our eyes. It was a time when the departments of neurology and psychology could be headed up by the same person, before accurate conduction studies to map beleaguered nervous systems, before the electron microscope let us see our enemy up close. (The poliovirus was first imaged in the early 1950s.) When we were so desperate not to acknowledge our helplessness in the face of this wayward force of mother nature that we injected patients with paralytic poisons and the blood of other victims in an attempt to arrest the progress of the disease. It was not a time when logic, as we understand it now, ruled the day.
But understand this, too: we didn’t even know most of these things for sure, back in the forties and fifties, when this terror opened up communities like it was ripping out a seam, warping the pattern of everyday life, exposing the fragile, private lining from which we tried so hard to avert our eyes. It was a time when the departments of neurology and psychology could be headed up by the same person, before accurate conduction studies to map beleaguered nervous systems, before the electron microscope let us see our enemy up close. (The poliovirus was first imaged in the early 1950s.) When we were so desperate not to acknowledge our helplessness in the face of this wayward force of mother nature that we injected patients with paralytic poisons and the blood of other victims in an attempt to arrest the progress of the disease. It was not a time when logic, as we understand it now, ruled the day.
These patients—these kids, mostly—didn’t care what was going on in the deepest reaches of their cells. It’s disingenuous to say that we shouldn’t either—that’s why I told you all about it. But it tells us nothing about the things that really matter: the brutal contagion of fear, the stigma and terror of isolation, the pain and the stares and the shame. The details are interesting mainly in that they are so brutally indifferent, and we are so much at their mercy. The details are almost insulting.
What polio was is a notion utterly divorced from what polio was like.
And now that we’ve covered the basics, it’s time to delve a little deeper.
26 Friday Apr 2013
Posted in Introduction
Tags
The syrupy exhaustion descends a little at a time, a slow slide of the dimmer switch on the world, darkness fogging your thoughts. The world seems suspended, or maybe that’s you—something’s off about your relationship to the ground. Gravity isn’t working quite right, and it’s making you dizzy, and you can’t remember what you’re scared of. You’re drenched in clammy sweat, even though that doesn’t make sense, because the droplets are running off unevenly, pooling in between the constellations of goosebumps on your skin. There’s a miserable knot in your stomach, and your limbs are filled with shifting sand. The pressure tightening around your temples has such physical weight it feels like you should be able to shake it off, but when you try the pain just clamps down harder.
It’s 1940, and you are inside your worst nightmare, and you’re afraid to even tell anyone, for fear of what they’ll do.
We hardly remember what the word means, now, but for fifty years, from the turn of the twentieth century to just past its midpoint, there was nothing in the world more instinctually terrifying than the specter of polio. More permanent than the Depression, more personal than any war, it had the power to upend lives almost overnight, transforming healthy citizens into weak, cramping phantasms, struggling for breath. Once the illness began, there was virtually no treatment, and certainly no cure. No way to know who would escape unharmed, who would be paralyzed, who might lose their life.
Polio victims left home in ambulances, and they came back transformed. Whether or not they returned in wheelchairs, supported by crutches or canes or the heavy metal leg braces that for so long functioned as cultural shorthand for the disease, they were newly burdened, weighted, in a way no one else seemed quite able to fathom. And that metamorphosis held an entire nation in terrified thrall.
Because polio changed people. And not just on the outside.
We have—and, especially, people had then—this preconceived notion that being disabled isn’t supposed to change you as a person. It seems rude, somehow, to assume that someone with significant physical challenges differs from able-bodied people in matters beyond the simply practical, and offensive to suggest that they are really other, that they see the world differently.
But they are. Different. They are different in the same way as all of us, shaped by their experiences—and those experiences, especially in the 1930s and 40s, bore little resemblance to those of the unafflicted (to use a contemporary term). They spent weeks in dark isolation wards, separated from their families, foggy from the brain infection and largely ignored by their doctors. Inpatient rehabilitation lasted months or years, sometimes in gentle kind places, sometimes in militant, miserable ones. Some endured dozens of surgeries; others were subjected to draconian therapy regimens that involved months in body casts or strapped in rigid splints. All went through unspeakable pain—physical pain, and the pain of loss, which feels no less agonizing, and hardly less concrete.
 This disease laid people bare, shaken and shattered, and even those who beat the odds to walk back into the world unencumbered had to find a way to rebuild from the trauma. Some changed for the worse; others, in the end, perhaps for the better. Who each person became depended on who they were to begin with, and how they were treated, and the people they met on their strange and sometimes devastating journey. And even at the time the public gawked like spectators at a zoo, trying desperately to wrap their heads around the horror, unable to see it the way the survivors themselves did: as everyday, dogged reality, sometimes inspiring, sometimes bleak, never predictable.
This disease laid people bare, shaken and shattered, and even those who beat the odds to walk back into the world unencumbered had to find a way to rebuild from the trauma. Some changed for the worse; others, in the end, perhaps for the better. Who each person became depended on who they were to begin with, and how they were treated, and the people they met on their strange and sometimes devastating journey. And even at the time the public gawked like spectators at a zoo, trying desperately to wrap their heads around the horror, unable to see it the way the survivors themselves did: as everyday, dogged reality, sometimes inspiring, sometimes bleak, never predictable.
By the sixties, just a few short years after the advent of Jonas Salk’s famous vaccine, we’d forgotten any of this had ever happened.
I have written and rewritten this segment a thousand times, because I don’t want to fall prey to the reductionism you see in so many other dealings with the topic. Because I want you to hear this story the way that I do, see these people the way they really were. I want to tell you what really happened, insofar as I can find that out, not tell a story about what happened: the things that transpired here form neither a comforting narrative of triumph nor a sensationalized story of pain. It’s just a story, about people, and about those who tried to take care of them. It’s a story I think is worth remembering. Something that still informs our national attitude of determination and bravado, for better or for worse. Something I think we shouldn’t lose sight of.
But we have lost sight: of the tremendous impact of this part of our history, and the fact that it happened at all. I read an interview once, in a remarkable compilation of first-person accounts called Polio’s Legacy, in which someone recalled being asked by younger neighbors if his children were “okay;” presumably they thought that the “polio” that kept him in leg braces was hereditary, or somehow still catching.
We haven’t forgotten polio simply because we have the luxury of ignorance, or because the problem is obsolete. We forgot because we pushed it from our minds. We beat it, this terrible thing that stalked us for so many years, and so why should we acknowledge it? Why dwell on a nightmare after the waking?
It’s not accurate, exactly, to say we don’t talk about polio at all, or that people don’t think it’s important. Dozens of books have been written about it; David Oshinsky’s Polio: An American Story won a Pulitzer prize when it came out in 2005. We still talk about the disease plenty when we discuss the FDR presidency, or the ongoing vaccination debate (ask me how I feel about that sometime). But when we look back on it as a historical phenomenon, what people focus on is the race for a cure through prevention, our victory over polio, or else the sheer faceless horror of the disease. They rack up numbers of cases and children left helpless and paralyzed; they talk about the economic burden of the disease, or the hysteria it engendered. They talk about polio as a phenomenon. They talk about polio as an all-consuming fear.
They don’t talk about polio as something that happened to people. We lose track of our humanity, in those breathless chronologies, maybe because we are ignorant, or maybe because we’re afraid.
It’s not much different than it was at the time, when polio was still a scourge to be dreaded, and smiling poster children solicited donations on every corner while the survivors themselves stayed home, cast out for the unavoidable reality of their braces and canes, and the fact that they didn’t always grin. It’s easier to think about the macrocosm of war than about each individual battle. Wars can be won; it’s in the trenches that we pay the price for victory, and unless you’ve been drafted, it’s an easy fact to overlook. Behind each clinical sentence in a history book, or the bulleted list of symptoms on the Mayo Clinic web site, is, or was, a human being.
Teens and young adults were uniquely suceptible to paralysis, a pretty widely distributed fact, but the fact itself doesn’t address the sixteen-year-old who hugged her limp knees in bed, wondering if anyone would ever want to marry her, wondering if she’d ever make love. Discussions of the extreme (but ineffective) isolation measures never speak specifically of the parents who circled the outsides of hospitals until they found their child’s window, because during an epidemic a knock and a wave was as close as they could get. Knowing how much money the March of Dimes spent on splints doesn’t give us a chance to ask how they made the boy who laid for months with his arms at right angles feel. Iron lungs had children in them—children who sometimes dressed them up in Halloween costumes.
Every single time I talk about my project, this project, each time I reach out to shake a new hand, I hear another story. It pours out of people like something pressurized too long: My dad had polio, they’ll say. Or My grandmother. Their eyes go wide, and a weight lifts as they soften, like it’s good to say it, like it’s a relief to talk to someone who knows what they’re talking about. The boy down the street was in an iron lung.
I had polio, they say, sometimes, quietly. And then, always, some variation on Wow, because even—maybe especially—for the people I’d never have guessed that about, the ones who seem physically totally intact, the reminder has its own gravity. Its own power to turn back the clock.
There are plenty of things about myself I don’t usually share; some of them happened an awfully long time ago, long enough that hardly anyone knows. And every single time I get close to someone, there comes a tipping point in the conversation, a threshold where I want to say it, but I don’t, usually, because it isn’t really relevant, except in that space inside my head that begs for a voice. Just because you can’t see it doesn’t mean it didn’t change me. Just because it doesn’t “matter” to whatever we’re discussing right now doesn’t mean there isn’t some part of me that wants you to know.
I feel incredibly lucky to hear those stories from others. To be the one entrusted with them, at least for that fleeting moment. Maybe people don’t talk about it because they imagine it won’t interest anyone, or because they’re still afraid of censure, or maybe it just doesn’t occur to them, in the rush and reality of everyday life. But there is a void there. There is something left unsaid. I see it almost every day. It’s a void I don’t think anyone else is trying to fill.
It’s a void that was filled at the time mostly by a remarkable and enigmatic woman named Elizabeth Kenny. A nurse from the rural Australian bushlands, her unique regimen of treatment for the disease not only revolutionized the field of physical therapy but changed her patients forever, in a way that entirely transcended their mobility. Conventional wisdom about polio held that paralysis was absolute, and that exercise was dangerous, with passivity the only possible source of redemption. She rejected that worldview completely, insisting that not all weakness had to be permanent, that helpless submission to the medical machine wasn’t necessarily the appropriate response to the situation, and that imperfection shouldn’t bring with it a secret shame—and her method worked beautifully. Doctors hated her. Patients loved her. And she didn’t seem much fussed either way.

Back in 1940, when Kenny first stepped onto U.S. soil, she was entering into a society that liked its brave, idealized concept of polio survivors a lot better than it liked the real thing. The medical institution was filled to bursting with doctors who felt existentially threatened, unable to cope with their helplessness in the face of the disease. They treated their patients as collections of muscle-testing results and constellations of symptoms, because to acknowledge their humanity would mean acknowledging their suffering. And acknowledging their suffering would mean acknowledging they’d failed. So they pushed them harder, straightened their twisted limbs with ever-increasing violence, so that they could be closer to normal, and the tension could fade from the air.
For nurse Kenny the very idea of allowing those kinds of metrics to define a patient, a person, was anathema. She, too, saw the intrinsic humanity in her patients, and she wanted for them true recovery, rather than some objective standard of performance. She was more interested in how her patients felt than in how far they could or couldn’t walk. And she knew, that to ever get better—whether better meant walking unassisted, or better meant self-acceptance—honesty and wholeness, rather than some fragmented medical identity, was what was required. Her therapeutic technique was what earned her recovery rates more than twice the average of the day. But it was her therapeutic philosophy that left her patients filled with admiration rather than fear, and inner peace instead of self-reproach.
It wasn’t a person’s life you feared for when they came down with polio—it was their ability to live. And even if she couldn’t repair a broken body every time, it was in assuaging this fear that Elizabeth Kenny healed. It’s a tremendous story of persistence and triumph and hope, and a terrible one, too, of prejudice and darkness and inalterable loss. It’s a story that has more to do with the scars you can’t see than the ones that you can. And I’m in the process of writing a book about it, and her, and about the Minneapolis clinic where she did her best work—the book this site is intended to accompany.
I’m not the most logical steward of this story. I’m twenty-one years old, born the year the Kenny Institute celebrated its fiftieth anniversary. I run marathons and listen to cringeworthy pop music; my laptop is grafted to me like a third limb, and my hair is sometimes dyed firetruck red. But I’ve been fascinated by this story for a long time, and I believe it desperately needs to be told. So I’m taking comfort in this: Elizabeth Kenny—almost six feet tall, self-taught, and frequently lacking in social graces—was not an especially logical hero.
I can’t wait to tell you more.


{kind=link}
{kind=link}