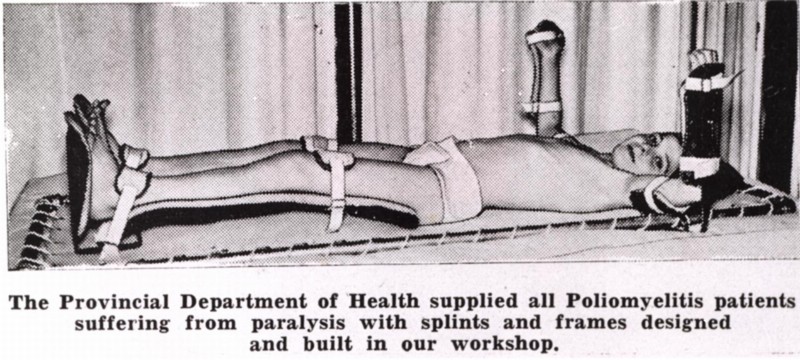
There is a lot of amazing stuff, in the stack of ludicrously heavy filing boxes that make up the Minnesota Historical Society’s “Kenny Papers.” But one of the more arresting parts of the collection is a thick folder of letters, newer than most of the things housed there, and without their musty smell and air of fragility.
Some of the letters are written by hand, in the beautiful looping calligraphy kids don’t learn anymore; I certainly couldn’t replicate those effortless, soaring curves. Others are tapped on typewriters, or printed in erratic monospace font, spat out unceremoniously by early word processors. They come on paper of every imaginable color and size, some intricately folded, others not at all. There are short ones, barely a paragraph, and ones that seem to go on forever, and it’s obvious that none of them say anywhere near as much as they could. Some are creased razor-sharp, the lines so straight they seem to have been written across a ruler; others sprawl and squirm, thick paper rippled by moisture, the residue of sweaty hands or falling tears.
I’d swear that even after all this time–exactly as many years as I’ve been alive–some of them still carry a faint whiff of elegant perfume.
They’re letters written about the still-extant Sister Kenny Rehabilitation Institute on its 50th anniversary in 1992, when a prominent Minneapolis newspaper asked former patients to contribute their memories of the time they spent there. And the differences are semantic, because the content of every single one is the same. I’ve never seen the initial request, but it must have been restricted to the very earliest patients, from the forties and very early fifties, the ones who knew Sister Elizabeth Kenny personally. Or maybe they were simply the ones who felt moved to write in en masse.
The letters are incredibly, unreservedly warm, and to a one palpably grateful. These people, fifty years later, remembered their time at the Insitute—or “Kenny,” some of them called it, “my time at Kenny”—with nostalgia almost unto joy. The time they had spent as inpatients in that squat little building in the heart of Minneapolis was time they’d come to treasure. And they wanted, so exuberantly, so delightfully, to tell their stories. To explain how their brimming, happy lives had played out, and thank everyone involved, even though so much time had gone by that most of the Institute’s original staff had passed away.
It’s fantastic. There really isn’t any other word for it. I came to these things after months immersed in the kind of desperate material I spoke at length about in the last few posts, a world drenched in fear and viewed perpetually in the negative: with the deep pessimism of resignation, and in garish, otherworldly colors. I saw none of that here. And what I saw instead enchanted me.
Who in the world was this woman, I wanted to know, and what was so different about this place?
As it turns out…that depends very much on who you ask.
Even though I’ve been researching her story for upwards of a year now, I’m still trying to tease out fact from fiction, and half-truths from the ones so complete they’ve been embellished into legend. It’s one of those stories, the best kind: where the most hyperbolically ridiculous statements are the ones most likely to prove true, and the ordinary things, the ones that establish a simple, everyday rhythm of life, are the toughest to pin down.
The lives of extraordinary people aren’t so different from anyone else’s, day in and day out. But those aren’t the things people remember.
 Born in 1880, Elizabeth Kenny grew up in rural Australia, part of a large, rambunctious family with a formidable number of children. Easily the most fearless and outgoing member of an already free-spirited group, when she broke her arm as a teenager, she convinced the doctor who set the bone to take her on as an apprentice. (Though she would later claim various nursing certifications, this may be the only supervised medical training she ever got.) After a couple of years spent working on and off for Dr. McDonnell, she ventured out on her own to serve as a “bush nurse.” It was somewhere in the depths of these years, making house calls on horseback to families who lived dozens of miles from anything approaching “civilization,” that she started treating polio cases.
Born in 1880, Elizabeth Kenny grew up in rural Australia, part of a large, rambunctious family with a formidable number of children. Easily the most fearless and outgoing member of an already free-spirited group, when she broke her arm as a teenager, she convinced the doctor who set the bone to take her on as an apprentice. (Though she would later claim various nursing certifications, this may be the only supervised medical training she ever got.) After a couple of years spent working on and off for Dr. McDonnell, she ventured out on her own to serve as a “bush nurse.” It was somewhere in the depths of these years, making house calls on horseback to families who lived dozens of miles from anything approaching “civilization,” that she started treating polio cases.
The story of her very first encounter with the disease is a great one, and I won’t tell it here, at least not right now. But the crux of the story is contained in a single telegram sent by Kenny’s mentor, after the young, terrified nurse reached out for help.
“Infantile paralysis,” Dr. McDonnell told her. “No known cure. Do the best you can with the symptoms presenting themselves.”
And so Kenny did—and her young charge made a full recovery, along with the half-dozen others who fell ill in the outbreak. She had no idea what you were “supposed” to do with polio patients, or even what was assumed to be wrong with them. It’s a big leap, actually, from “this patient can’t move so well” to “this patient is paralyzed,” and in circumventing the conventional wisdom—not because she was rebelling against it, but because she didn’t know what it was—Kenny found loopholes and inconsistencies in that thinking that led her to an entirely different method of treatment. Among other things, gentle exercise took the place of immobilization, and intense heat therapy stood in for bizarre drug injections—and the results were spectacular. (I am being, here, intentionally vague; a further explanation of these competing treatments, and the way Kenny’s approaches to neurology and psychology intertwined, is in the pipeline.)
With a couple of brief detours into other endeavors, Kenny worked from that point forward rehabilitating people with disabilities who had been written off as hopeless—not just polio patients, but also kids with cerebral palsy and other neuromuscular disorders. As word of her method (and its effectiveness) spread, so did the controversy: she claimed to observe dramatically different symptoms than had been recorded by anyone else, the symptoms on which her method was based, and an air of self-righteous indignation started to gather around her.
One of my very favorite lines in her (spectacularly funny, and spectacularly fictionalized) first autobiography, published in 1943, tells you pretty much everything you need to know about her manner of interacting with others: “Some minds,” she says, “remain open long enough for the truth not only to enter but to pass on through by way of a ready exit without pausing anywhere along the route.”
This was not a clever aphorism devised to get a smile out of readers. It was a philosophy by which she lived, and if she thought you suffered that particular affliction, she was not shy about telling you so. A contemporary journalist might have called her the “Angel of the Outback,” but Elizabeth Kenny was hardly a saint. (Nor was she a nun, despite being widely known as “Sister” Kenny; that was a title bestowed upon decorated nurses in the Australian army, where she served during the First World War.)
 Part of the reason I decided to do this project is the frequency with which people still try to discredit Kenny, on the rare occasions when the story is dragged out of the historical attic, and that modern prejudice is rooted in the ferocity of the original controversy. Doctors loathed her, almost to a one, because everything about her rankled—her gender, her lack of credentials, the fact that she said they were wrong—and when they rebuffed her, she pushed back with equal ferocity. She was right, obviously, and everybody else was not only wrong but also incredibly stupid. (This is a diplomatic strategy that tends not to further negotiations.)
Part of the reason I decided to do this project is the frequency with which people still try to discredit Kenny, on the rare occasions when the story is dragged out of the historical attic, and that modern prejudice is rooted in the ferocity of the original controversy. Doctors loathed her, almost to a one, because everything about her rankled—her gender, her lack of credentials, the fact that she said they were wrong—and when they rebuffed her, she pushed back with equal ferocity. She was right, obviously, and everybody else was not only wrong but also incredibly stupid. (This is a diplomatic strategy that tends not to further negotiations.)
It wasn’t until 1940 that she landed in the United States, and there’s some confusion about why she ended up here in the first place. To hear her tell it, she was sent by the Australian government and its public health counsel to spread her technique as a point of pride for her country; less generous accounts sometimes imply that they wanted very badly to get rid of her. But after unsuccessful presentations at hospitals in New York and Chicago, just as she was about to return to Australia, she met a duo of sympathetic doctors from the University of Minnesota hospital…and it was in Minneapolis that the other side of the story blossomed.
Kenny might have been combative with doctors (and, when necessary, politicians, the press, and her own staff). But to her patients, she really was something like a saint. Gentle and attentive, she was their constant defender from a system that didn’t take them any more seriously than it took her. They became co-conspirators, in a way, and it was an arrangement that seemed to strengthen everyone involved. Kenny didn’t have time for anybody’s—well, it’s not exactly a family-friendly word. But she always had time for her kids.
Russell Papenhausen, the gentleman I interviewed a few weeks back, who I’ve mentioned a couple of times, lights up when he talks about her. At age fourteen, he was one of her first patients in Minneapolis, treated before the Kenny Institute (her very own 80-bed hospital, founded in 1942) even existed. And he put it more simply, and with more authority, than any of my pretty words ever could.
“She was a marvelous woman,” he told me, breaking into a mischievous smile. “She put the fear of Christ in the grownups and nothing but love in the youngsters.”
 This was the one time that the patients’ voices won out, and, almost overnight, the beleaguered nation fell in love. Everyone in a position of prominence during the height of the polio epidemics gathered around them many dozens of sycophants; Basil O’Connor, the (extremely reluctant) director of the March of Dimes, was lionized by many, chief among them President Roosevelt. But not many people had letters sent to them asking, in all seriousness, “Would you let me know when it would be practical for you to receive a 15 lb. ham?”
This was the one time that the patients’ voices won out, and, almost overnight, the beleaguered nation fell in love. Everyone in a position of prominence during the height of the polio epidemics gathered around them many dozens of sycophants; Basil O’Connor, the (extremely reluctant) director of the March of Dimes, was lionized by many, chief among them President Roosevelt. But not many people had letters sent to them asking, in all seriousness, “Would you let me know when it would be practical for you to receive a 15 lb. ham?”
A reporter named Inez Robb wrote the following, after her first visit to the Institute, with the breathless lack of objectivity endemic to midcentury journalism:
When I went out to the institute, I went up to visit a patient in the big ward which houses 29 boys ranging in age from 6 to 16. When I came into the ward, I saw a sight that stopped me in my tracks. Two lively kids of seven were wrestling vigorously in a hospital bed. It was a rough and tumble scrap.
At that moment, the nurse reappeared.
“Tommy! Johnny!” she said authoritatively. “Stop that at once! Tommy, you know you are not allowed out of bed. Get back into your own this instant!”
The kids looked sheepish. Tommy, a beguiling imp with big black eyes, got back into his own bed.
“Kids have so much pep,” the nurse said. Kids with infantile paralysis with pep! With too much pep!
“It seems like a miracle,” I said helplessly.
Kenny hated the word miracle—because it embarrassed her, she always claimed, and because it wasn’t true; I suspect it had more to do with the fact that it gave God credit she would have preferred to keep for herself. But of course it seemed like a miracle. It seemed like a miracle to the uncountable, unfathomable number of parents who had been told their child would never walk again, and to the children who’d believed their lives were forfeit—but for very different reasons. In her baker’s dozen years in America, Kenny tiptoed, and sometimes blithely trampled, the vanishingly thin line between what society expected from a great healer of polio victims and the kind of compassionate care those people actually needed.
Kenny was beloved by the nation for the results she produced: the Kenny Institute’s recovery rate was vastly greater that of any other treatment facility’s—about three times higher than average. More of her kids walked; eventually some ran and jumped and fought for our country in the Second World War (including my new friend Russell). Few wore braces or endured the spinal curvature common among polio survivors; if they used crutches, they were the short forearm type known then as “Kenny sticks,” rather than the awkward underarm variety, the kind you were supposed to use when you broke an ankle, and which gained an extra sense of pathos in their permanence. The science, however controversial, was sound; the therapy worked. Kenny’s kids got better.
But her patients didn’t love her because she made them well. They loved her because—against all odds, in a situation just once removed from the fires of hell—she made them happy.
 I think my favorite thing in the Kenny papers—more touching than the huge box of thank-you letters, more chaotically revealing than the hundreds of disorganized photographs—is a box of newsletters, crudely typewritten sheets the patients at the Institute put out at various intervals in the 40s and early 50s. They were sent out to kids’ families and circulated inside the clinic, blurry duplicates on brightly colored sheets of cardstock, rife with good-natured ribbing and inside jokes. The young writers gossip innocently about their therapists and doctors and nurses, gush about the photography classes they’re taking or the movies brought in for them to watch, speculate about what they’ll do when they get out, who they’ll be when they grow up. They tease with enthusiasm old friends who come back for outpatient visits, especially when their subpar performance in the checkup meant they’d have to come back for a kind of remedial stay.
I think my favorite thing in the Kenny papers—more touching than the huge box of thank-you letters, more chaotically revealing than the hundreds of disorganized photographs—is a box of newsletters, crudely typewritten sheets the patients at the Institute put out at various intervals in the 40s and early 50s. They were sent out to kids’ families and circulated inside the clinic, blurry duplicates on brightly colored sheets of cardstock, rife with good-natured ribbing and inside jokes. The young writers gossip innocently about their therapists and doctors and nurses, gush about the photography classes they’re taking or the movies brought in for them to watch, speculate about what they’ll do when they get out, who they’ll be when they grow up. They tease with enthusiasm old friends who come back for outpatient visits, especially when their subpar performance in the checkup meant they’d have to come back for a kind of remedial stay.
Because, the authors declared, only half joking, they knew nobody ever really wanted to leave.
I find myself holding my breath while I read them, like suspending the present can take me back in time, or like if I wait long enough or attend closely enough I might be able to inhale the stale air, with its sweetly rancid scent of rambunctious kids at play. There’s plenty of irony in the Kenny Stretch, and more than a little dark humor, but hardly anywhere do you see a forced smile. Isn’t this such a weird, messed-up world we live in? they ask, unselfconscious, and wise beyond their years. Isn’t this awful? Aren’t we bizarre?
Yes. And gloriously so. Because their lives belonged to them, and them alone, and it’s clearer here than anywhere else. Nobody else got to decide how they felt, or what they were afraid of. They might have been far from home, stranded apart from everything they knew or understood, but this new world was one they were building themselves.
The Kenny Institute was no less of a microcosm than any other inpatient facility—more so, actually, with its tight restrictions on visitors, and conspiratorial sense of community—but it wasn’t a place where you waited for your life to start up again. It was a place where you celebrated the life you still had, the one you were living, because someday was far away, and you were still exuberantly breathing right now. Though she never stated it explicitly herself, it’s obvious that it wasn’t just Kenny’s therapeutic concept that differed from the norm. Her philosophy was wildly different, too, and its core postulate was this: that recovery wouldn’t happen unless you were deeply invested in it yourself, and that in order to be willing to sink such physical and emotional effort into an outcome that was ultimately so uncertain, you needed to value yourself right now.
Her patients had to understand what they were working for, and that that work was something they did for themselves. Not for some anonymous coalition of doctors who poked and prodded at your limbs and scribbled down incomprehensible numbers on a chart, who wouldn’t tell you if you failed. Not for parents who worried that a lingering disability meant giving up on everything they’d hoped for you in life—not to mention what the neighbors would say, or how the checkbook would balance. Not to keep up with siblings or friends or an amorphous notion of what it meant to have dignity.
And—perhaps most importantly—not even because Sister Kenny told you to. Sister Kenny was not afraid of telling you to, and in no uncertain terms, but—unlike pretty much everyone else in the rehab community, at least according to the patients whose accounts I’ve read—she wouldn’t make you do much of anything at all. If you couldn’t prioritize your own recovery, couldn’t take the initiative to focus on getting better—which meant deciding that getting better mattered, which in an uncertain world must have meant you mattered, at least enough to try—she knew she couldn’t force you to succeed, any more than those stubborn doctors could force her to shut up.
You couldn’t just choose to get better.
But you could choose to live.
Put even more simply: “back to normal” wasn’t under your control, or, however skilled her hands and gilded her reputation, Sister Kenny’s. Recovery depended on factors no doctor or therapist could possibly foresee, on the degree of stripping in the wires, on the strength and stubbornness of your body. But better—partly in the sense of performing “better,” to whatever degree you accomplished that, but also partly in the sense of feeling better, feeling safer, more whole—that was a choice. And it was one you had to make; no one one else could make it for you.
That kind of responsibility was terrifying, especially to kids coming out of hospitals where they’d been treated as all but inanimate. But it taught them to stand up straight—in more ways than one—without feeling like they were being puppeteered. Not everybody remembers the Kenny Institute as a wonderful place to be, and it wasn’t an unconditional blessing for anyone. The reality of this situation was impossible to ignore—even if it was, eventually, possible to escape—and patients were asked to face it head-on far more often under Sister Kenny’s care than at most other facilities. The physical and psychological demands she placed on children widely believed to be both incredibly fragile and uselessly damaged were enormous. But those expectations were also an endorsement of personhood, and a gesture of respect, and for even the youngest of her patients, those confidences were transformative.
“You were lucky,” Russell’s wife told him, at the end of our second interview, after we’d fallen silent, exhausted, companionably sharing a plate of homemade cookies she’d brought.
He looked up, quizzical, in the middle of a bite.
“Not lucky to have polio,” Andree amended, waving a hand. “But lucky she came along when you did.”
It was exactly the same sentiment expressed by the wire-service reporter I quoted earlier, in a different, later piece: the children of Minneapolis, at that particular juncture of history, were the “luckiest in the world.”
Not because they were safe; nobody in the world was that, in the midforties, from polio or anything else. Not because there was nothing horrifying about their world, or because that world was free from danger. Because they had the thing that we all so desperately need, and that so much of the rest of the country at that point lacked.
They had hope. And more than hope, they had agency: the courage to find their own voice, and the fortitude to know that the only way to keep their illness from defining them was to write that definition themselves, before anyone else had a chance.
 This is the story I’m telling. And this is “A Louder Silence”: the embrace of volume, and clamorous voice, in the midst of a world determined to strip away all the noise. The chattering static of undisguised reality, and the way it starts to sound like music, if you tilt your head just exactly the right way. And the other kind of silence, lurking underneath such fearless self-expression: the ability to sit quietly inside yourself, to find some kind of peace, without needing to thrash away at endless, anxious insecurities. To shout with joy, rather than defiance.
This is the story I’m telling. And this is “A Louder Silence”: the embrace of volume, and clamorous voice, in the midst of a world determined to strip away all the noise. The chattering static of undisguised reality, and the way it starts to sound like music, if you tilt your head just exactly the right way. And the other kind of silence, lurking underneath such fearless self-expression: the ability to sit quietly inside yourself, to find some kind of peace, without needing to thrash away at endless, anxious insecurities. To shout with joy, rather than defiance.
Of course, it’s not always that easy. It’s probably never as easy as I just made it sound. But it was possible. It was beautiful. And this silence deserves to be amplified.
Welcome home.