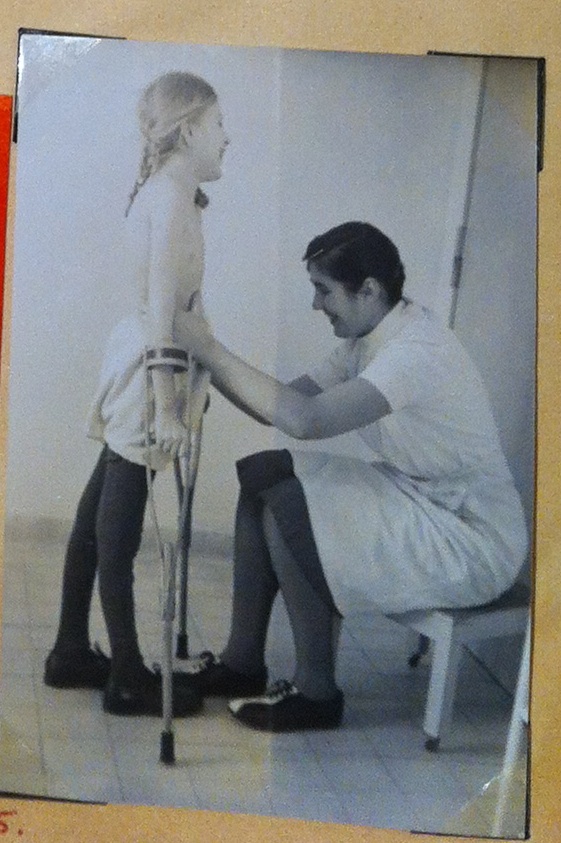
She is grim and anxious, captured in this set of black-and-white photographs. Her small body rigid, she stands barely balanced on a pair of short forearm crutches, mouth set and sharp as a razor blade. You can see how much she needs this step, and how hard her heart must be beating, keeping time with the shaking of her weak, tangled muscles as she moves. Her therapist’s hands are light on her slender legs, her ankles and calves, moving them forward one at a time, showing her where to go, making the effort she is still too wrung out to manage by herself. Her short hair is neatly braided, pretty and incongruously ordinary against the back of her neck. She’s maybe eight years old, or a little older than that, and she looks exhausted already, holding the weight of the world in her small hands, eyes fixed straight ahead.
And then something changes. I don’t know what happened in that moment, in the flicker of time between those shutter flashes (if shutters, or flashes, were even things cameras had back then). I wish I could have been there, to see exactly what elapsed between the fourth and fifth snapshots. But whatever it was—some whispered word of encouragement, or some feeling of triumphant familiarity—looking at that last picture is like watching the sun come up. Standing there, laughing, she is radiant on those crutches, this skinny grade-school girl. Elfriede Kohler is the happiest person in the world.
The day I saw that picture was the day I started to understand. What I was really looking at, and what someday I would be writing about, and what it would come to mean, and the ways that it would change me. Those photographs are the culmination of a lengthy scrapbook, lovingly assembled by someone at the clinic where Elfriede was treated, chronicling her progress from the depths of illness to partial recovery and discharge. The brown kraft paper is rippled and torn, and pictures have fallen out here and there, leaving tantalizing holes in the story that the handwritten captions don’t quite manage to fill.
And I sat there in the library, feeling the weight of this book in my lap, as fragile and enduring as the girl it preserves, and I knew I never wanted to give it back. Not just because the feelings were so profound. Because—at least in part—I was starting to grasp just how incredibly rare they were.
Moments like Elfriede’s don’t come along very often, in these stories, but even when they do, they sit far down the line from the place we left off. The illness was a dark, purgatorial space, after the before but just before the after, and no matter who you were, and what you might eventually achieve, the earliest forays into this new, unstable life were as terrible as anything that preceded them.
Polio’s paralysis is strange and unpredictable: its boundaries are fuzzy, its consequences vague, and, at least at the beginning, its permanence unclear. Weakness powerful enough to put someone in an iron lung could abate entirely within weeks, but someone else’s comparatively inconsequential limp might never get better at all. The effects are hardly ever symmetrical, nor are they especially well-contained: one side of the body is almost always much more heavily involved than the other, and even devastated limbs usually have some muscles that still work.
Even more uncannily, for all the glittering pins and needles of the illness itself, once the infection clears, sensation is rarely ever affected. So much of the world stays intact: the feel of the damp sheets against your body, the nurses’ rough handling of your tight, aching shoulders, the bright-lit pain that still pulses through your body, random and blinding as lens flare. It’s only your ability to interact with it that changes.
It doesn’t make sense, the straining that happens inside you, and the cruel disconnect between what you feel or imagine to be possible, and what you find really is. Some people talk about a sense of disembodiment, like that part they can still sense but can no longer command or comprehend doesn’t even belong to them anymore. More often, though, in recounting their experiences, people don’t talk about it at all. They are lying desperately ill in the contagion ward, and then they are in therapy, transferred somewhere else to reboot, to get better. The transition is so fast and so disorienting, and the things on either side of it so bold, that it doesn’t even stand out.
Every so often, someone will bring it up, often a little dreamily, like they’re only just realizing it’s true: I guess that was the last time I walked on my own.
Knowing seems to bring them comfort.
It was clear right away that something was terribly, terribly wrong, but it often took a long time to figure out just what it was. The moment it was possible to endure being touched again, the doctors swarmed back in—more often than not to contain you, compress together all your pain and confusion and complicated feelings and literally bind them to your body. Not just weeks but months of recovery were spent lying strapped down in bed, in an attempt to prevent further damage to weakened muscles. Infants were put into body casts; older children and adults found themselves racked on “Bradford frames,” traction-like devices that held them stretched out, often with their arms at right angles.
“The immobilization is maintained for a period of eight weeks, a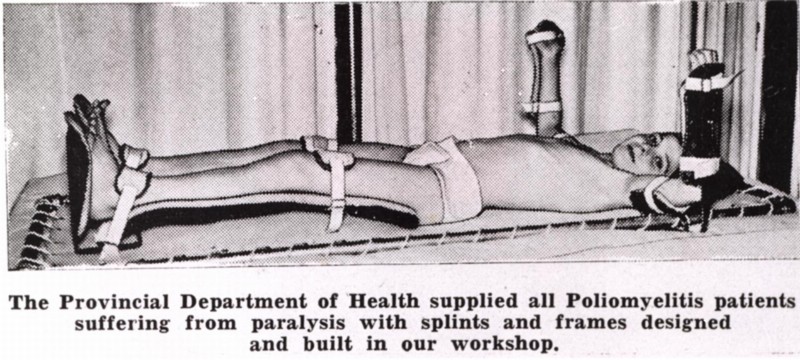 t which time a second muscle test is made…. If exceptional improvement is shown, this immobilization…is repeated,” a prominent 1941 textbook, Dr. Philip Lewin’s Infantile Paralysis, instructed. These eight-week periods were to be repeated indefinitely, but were “seldom continued for more than six to eight months.”
t which time a second muscle test is made…. If exceptional improvement is shown, this immobilization…is repeated,” a prominent 1941 textbook, Dr. Philip Lewin’s Infantile Paralysis, instructed. These eight-week periods were to be repeated indefinitely, but were “seldom continued for more than six to eight months.”
As if that’s no time at all. As if everyone old enough to understand what was happening to them didn’t use that time to think about what would become of them after all this was over. Didn’t lie in bed worried and helpless, and knowing all too well what would happen if it didn’t work. If they didn’t get better.
People don’t talk about the transition, and those early days and weeks of recovery. But they talk about the extremes to which they later went to fight for normalcy. They talk about being haunted by a stigma they were desperately trying to avoid.

There’s a poster that’s frequently reprinted in historical retrospectives of the “polio years;” I first saw it in a 2005 exhibition at the Smithsonian Museum of American History in Washington D.C. Created for a vaccination awareness campaign in 1956—the second summer the shot was available—it shows two different pictures, dramatically-split screened by contrasting backgrounds. On the right stands a smiling grade-school girl in tight buns that bear a passing resemblance to Princess Leia’s, balanced awkwardly on wooden crutches, the angle of her slender arms calibrated to imply even more deformity than she seems to suffer. On the left, two able-bodied children stride confidently through a field, wholesome hands intertwined.
This, the caption reads, above the happy siblings. Not this, above the bravely grinning girl. Vaccinate your family now
This. Not this. This. Not this.
This was the world the many thousands of people paralyzed annually by the disease in the U.S. alone had to live in.
Every single depiction of polio, every warning against it, characterizes the disease as a hideous specter, sometimes literally so: in a film called The Crippler, produced by the March of Dimes, the illness moonlights as a grossly elongated shadow, looming darkly over unsuspecting homes. Polio was horrifying, of course, and more than likely this visceral repulsion accomplished its objective: eliciting donations, raising awareness, and getting kids vaccinated, when that time came. But in associating the illness with the grotesque, its victims were tainted that way, too. As disgusting and contaminated, or else tragic and courageous, almost martyred, helpless young sacrifices to a noble cause. We put these kids up on pedestals even as we shrank from them in terror.
Having polio no more made you brave than it made you broken. It meant you were in the wrong place at the wrong time, that you shared the wrong ice cream cone or dove in the wrong swimming pool. The poster child was a cultural fantasy, not a reflection of reality.
But how do you understand that, at four years old, or fourteen? You’d seen those pictures, unless you’d been living under a rock since the day you were born. You knew what it meant, to have had this happen to you. And you knew that the only way to be okay again, to avoid being pitied or lionized, was to get better. All the way better. Even the kids in those posters knew it: “Help me walk again,” a picture of a child in a walker pled, and a happily skipping boy was triumphantly captioned, “Your dimes did this!”
Getting better became the only thing that mattered. The only way to feel real again. And not just getting better. Getting well.
In the mem oir Warm Springs, about her surgical rehabilitation at FDR’s famous polio hospital, Susan Richards Shreve recalls her younger brother asking if going in for reconstructive operations frightened her.
oir Warm Springs, about her surgical rehabilitation at FDR’s famous polio hospital, Susan Richards Shreve recalls her younger brother asking if going in for reconstructive operations frightened her.
“I’m not scared,” she told him. “The next time you see me, I’m going to be a different girl.”
“What kind of girl?” he asked her.
“A perfect one.”
It wasn’t just the specter of posters in shop windows and hyperbolic movie reels that made this seem so crucial. It was the reality you lived, day in and day out, in most inpatient rehab facilities. After the restraints finally came off, patients were often started on aggressive exercise regimes, hoping to strengthen them enough to get them back on their feet. The goal, always, was sitting, standing, walking, no matter how much supportive bracing that required, or how much it might hurt.
 The acceleration was dizzyingly brutal: kept from doing anything for so long, now you were expected to do everything, and the goal wasn’t really to make you feel better. It was to achieve something as close to normalcy as possible, no matter how strenuously your weakened body protested, and when inevitably you ran up against something you really couldn’t do, it felt like your fault. Like you’d failed somehow.
The acceleration was dizzyingly brutal: kept from doing anything for so long, now you were expected to do everything, and the goal wasn’t really to make you feel better. It was to achieve something as close to normalcy as possible, no matter how strenuously your weakened body protested, and when inevitably you ran up against something you really couldn’t do, it felt like your fault. Like you’d failed somehow.
And once those insurmountable roadblocks were found, the limits of your natural recovery defined—at least as far as the (misguided, but we’ll get to that) doctors were concerned—the next step certainly wasn’t acceptance. At a time when fighting to win at any cost—not just in the battle against polio, but in nearly every circumstance, great or small—was not only virtuous but expected, acceptance felt synonymous with giving up. Encouraging someone to come to terms with their disability was unthinkable: if the patients didn’t feel adequately distressed about how they were doing, what reason would they have to keep struggling?
The next step, instead, was surgery. Surgery to fuse bones, to transplant tendons from functional muscles to paralyzed ones, to shave down joints unhinged by muscle cramps. Dozens of surgeries, sometimes, stretched out over years, trying to account for growth, and the pernicious influence of time. For the most part, these procedures were designed not to make the patient feel more comfortable, but to make her more conventionally functional, closer to “normal”—whether or not that was something she actually wanted, or that her weakened body could support.
Lest you think I’m being hyperbolic, or exaggerating the extent to which recovery alone restored legitimacy, I want to share some excerpts from a March of Dimes pamphlet meant to “help” affected teenagers cope with the aftermath of their illness. There’s no date that I saw on this slender, seemingly innocuous document, but I’d bet anything it came from the mid-40s, with both fear and determination at their most histrionic peak.
“Everyone has problems to solve. Some are easy. Some are hard,” it begins, with an understatment that feels almost deadpan. “When you are ill your problems are more difficult to solve, more annoying, and many times you do not know where to turn for help.”
Then the language turns from merely patronizing to aggressively fraught with expectation: “it is…the function of the National Foundation to help you win your way back to health.” You and your family are “fighting to defeat the effects of the polio virus insofar as human skill and knowledge can do so”—and human skill and knowledge were held in high esteem at the time, with the country deep in the throes of new American exceptionalism, awestruck by unfathomable advances like the atomic bomb.
“If this little book does help you to ‘learn the score,’” the introduction concludes, “if it helps you become better able to conquer your polio and return to a full and happy life, it will have done everything we hoped it would do.”
There is no space, in that tone of enforced cheerfulness (which continues, blithely, through the rest of the booklet), for anyone whose recovery is less than triumphant. There are only winners and losers, without space left to to carve out a life in between—when life in between was most often the reality you confronted. No doctor ever asked a child when enough was enough, or how she felt about what was happening to her. They certainly never asked the darkest, and perhaps most crucial, question: Do you even want to get better?

It seems like an absurd thing to ask, doesn’t it? Of course you’d want to get better. There was nothing redeeming, hardly even anything tolerable, about this illegitimized existence, lost in the darkness of constant discomfort, at the mercy of a system you didn’t understand. But what the doctors failed to understand was this: rehab felt like a kind of limbo, a probationary period, where the rules and privileges of normal life were suspended. It was the place where you stayed while you waited to find out if your sentence would be commuted, and as long as you were there, everything else seemed far away. More often than not, the “real world” these kids were supposed to be fighting to rejoin seemed like nothing but a cruelly impossible dream.
It’s hard to convince yourself to work toward a goal with such a narrow definition. A difficult but attainable challenge is motivating. But it’s hard to imagine enduring that sense of futility, day in and day out. Lying in bed able to move just an arm, or a couple of toes, knowing that walking, that better, that normal, was the goal, made every incremental victory along the way seem less a triumph than an unbearable reminder of you how far you had to go.
Even if they couldn’t articulate it, there had to be some part of them that understood the paradox in which they were now unwillingly complicit. If you couldn’t get better, phyiscally speaking, but you had to get better, in order to win back your legitimacy as a human being, your right to take up the same space and breathe the same air as other people without inspiring revulsion or reverence, then what were you supposed to do? There had to be something you could do.
And there absolutely was: you could deny it.
Not that it had happened; that would have been absurd, not to mention impossible, for someone in a wheelchair, or encased in a body brace. But you could refuse to acknowledge that it had affected you. You might be in the chair, but the chair wasn’t a part of you. You were normal. It was your disobedient body that was the problem, and that didn’t really need to have anything to do with you. This whole thing was merely a formality, some kind of terrible joke, and you would reenter the world determined to prove that the real you was better than this chair you sat in.
At the end of the day, in order to be seen “just as yourself,” people felt forced to deny a huge, and hugely formative, part of who they had become. What had happened didn’t fit into anyone’s plan, or anyone’s image of what they wanted for themselves. But to refuse to alter that image at all, and to make a perpetual enemy of the crutches that held you up or the fingers that drifted uselessly at your side, created problems all its own. Insisting that you were unaffected, unchanged, un-limited, was an understandable reaction, but it was also a profoundly disingenuous one. Whether it came of the work ethic instilled in therapy, or developed as a defense mechanism to cope with the world thereafter, relentlessly having something to prove drove polio survivors to be—statistically!—much more accomplished than their healthy compatriots. But it also delayed, and in some cases denied, their ability to find peace.
I’m not implying that anyone failed, or that what anyone did was wrong: these attitudes were adaptive. Patients developed the skills they needed to live in a world that felt hostile and warped, out of line with all of their possible realities. They believed what their doctors and nurses and parents told them, and what kids don’t? What person doesn’t, under sufficient duress, cling to anything said with enough confidence and certainty? They needed a way out of the terrible place bad luck had landed them, and that way was better. At any cost. Better was a solid, straightforward goal. And that was comforting.
But there was another way.
It’s hard to give up that one clear goal, with its easy answers about who you are supposed to be and what you ought to want, and embrace uncertainty instead. It’s hard to accept things as they are, and keep picking your way across the river one rock at a time, turning with the currents of the water, neither frozen motionless in terror nor so desperate to push forward that the rapids sweep you in and pull you under. Rushing through the process was as impossible, and trying as disastrous, as lying back passively and giving up. It wasn’t just your “wholehearted cooperation and obedience when working with the physical therapist” (and doctors, nurses, and parents—again, according to the booklet) that made the difference. It was your ability to cooperate with yourself, and thereby learn to navigate the actual reality you lived in, rather than the one other people said you did.
It’s why I love that picture of Elfriede so much. What shines out through her eyes isn’t relief, or hope for the future, visions of what might come next. She isn’t dreaming of barefoot running or high school dances, or even setting down the crutches to stand on her own. She’s just happy. She’s found her feet again, and it feels amazing, and as far as she is concerned—she, and her grinning therapist, who seems equally delighted—in that moment that is enough. At that moment it’s everything.
That feeling—and the fact that it’s possible—is as rare and precious as her smile. The human spirit is astonishing, and it’s no surprise that some managed to evade the limitations pressed upon them, and navigate these labyrinthine preconceptions to make their way on strength of spirit—and an enduring sense of self—rather than pure force of will. There are plenty of beautiful stories scattered across the smooth, impassive surface of this seemingly unscalable edifice. But nowhere do they cluster as tightly as they do around Elizabeth Kenny—the nurse I mentioned in my first post, the one this book I’m writing is about—and the Minneapolis clinic she presided over for twelve years.
It’s not Kenny, in the pictures of Elfriede, which were taken somewhere on the outskirts of Germany, sometime in the early 1940s. But the young woman whose touch pulls the little girl forward into her moment of heart-stopping joy was a Kenny-trained therapist. And I’ve seen enough to know that what this mysterious revolutionary imparted to her charges—the therapists she taught, and the patients she treated—was as much philosophy as technique. And it came at a time when we all sorely needed a paradigm shift.
I’m looking forward to showing you around.