Tags
introduction, me, minneapolis, moving, present day, real life
Firstly: I owe you an apology.
It’s been almost three weeks since I’ve posted anything, and I didn’t mean to take so much time off from updating the blog. This site is a vehicle for many things—cheif among them educating people about my topic, and keeping them up on the progress of the project—and I’ve been delinquent in both of those arenas. Because there are things I haven’t told you, because I haven’t had a chance. Because I was yanked from something I thought I understood into something that became much more than I bargained for.
It hasn’t been an arbitrary silence, however sudden it might have been. But it was a quiet that fell without warning, I know. (It feels especially egregious to me to have left you all hanging in the wake of my emphatic, anthemic last post.) What to me has been three weeks more chaotic than any in recent memory has been three weeks of radio silence for you. A blank space, a mystery. A vanishing act. And, at least right now, at the beginning of this post, only I know where I’ve reappeared.
The story I’m telling is all about perspective. And so, for the moment, is mine.
A little less than three weeks ago—three weeks that feels like forever, a miniature lifetime not quite my own—I packed up my apartment in Chicago, and watched the past I knew vanish into two dozen cardboard cartons. I’d been considering a move since February, but it wasn’t finalized until April, and nothing felt real until it was happening all at once. Until the internet access clicked off, and the counters had been wiped down for the third time, and the keys were just lying there, on the table where I used to toss the mail.
 Three weeks ago, give or take, I threw my stuff into a U-Haul, and I came here. To this quiet house on a near-silent street, where on Sunday evenings no one breathes, and the sound of fingers on laptop keys bounces noisy off brand-new hardwood floors. A huge blackboard hangs on the wall, blank, for now, but raw with possibility, and on the floor a lamp beams out pale, softly colored light. It’s a grownup house, far more so than any I’ve lived in before, thoughtful in the way it’s put together, and the atmospheric statement it makes. I’m the one who made it that way, over three or four whirlwind days of trips to Target and IKEA furniture assembly, but there’s still something sort of bewildering about it. Something fragile and unreal.
Three weeks ago, give or take, I threw my stuff into a U-Haul, and I came here. To this quiet house on a near-silent street, where on Sunday evenings no one breathes, and the sound of fingers on laptop keys bounces noisy off brand-new hardwood floors. A huge blackboard hangs on the wall, blank, for now, but raw with possibility, and on the floor a lamp beams out pale, softly colored light. It’s a grownup house, far more so than any I’ve lived in before, thoughtful in the way it’s put together, and the atmospheric statement it makes. I’m the one who made it that way, over three or four whirlwind days of trips to Target and IKEA furniture assembly, but there’s still something sort of bewildering about it. Something fragile and unreal.
I live in Minneapolis now: a cozy two-bedroom on the outskirts of a neighborhood called Uptown, a few blocks away from Lake Calhoun. And the transition, which I thought would go so smooth and seamlessly, has changed me in ways I never could have imagined.
 It feels strange to take any part of the story I’m telling for my own, and to feel connected to it so strongly in the present, but it’s been very much on my mind in these last weeks. What it means to be sidelined by something unexpected, and to vanish from a world you share with others into a different one, a smaller one, where you find yourself both more and less alone. A world that can be terrifying, in the possibilities that bloom when you least expect them, when a path you thought was modest and well-defined branches out to dozens of possible successes and failures.
It feels strange to take any part of the story I’m telling for my own, and to feel connected to it so strongly in the present, but it’s been very much on my mind in these last weeks. What it means to be sidelined by something unexpected, and to vanish from a world you share with others into a different one, a smaller one, where you find yourself both more and less alone. A world that can be terrifying, in the possibilities that bloom when you least expect them, when a path you thought was modest and well-defined branches out to dozens of possible successes and failures.
Only so much of any intensely personal journey can be shared. There are limitations on words, ones I grapple with every day, in trying to illustrate the stories of people whose heads I will never entirely inhabit. (Nor is this challenge confined just to the problems of history; though I haven’t talked about it here, I’m also a fiction writer, working on a novel in tandem with this book.) I haven’t even defined them all for myself, the things that have changed since I came here, and that makes the seismic shifts even more difficult to articulate.
But I can say this, and easily enough: even with an overstuffed U-Haul, and all the things I brought with me, I left even more behind.
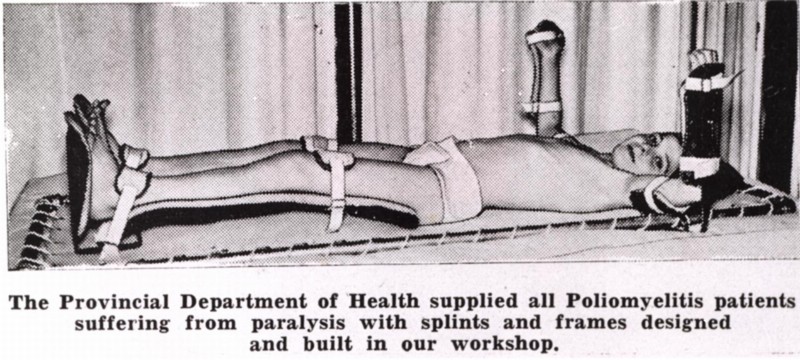
I came here to be closer to my research. To take the next step in teasing out the truth of the saga I’ve promised to recount, and get a better idea of how to go about the writing process itself. My apartment is a twenty-minute drive from the Historical Society in St. Paul, where they keep those archival boxes I’m always talking about, the ones that spill out stories like a thousand points of light. The site of the original Kenny Institute, the building stripped of its façade (and its purpose), but still recognizably connected to the one in the photo at the top of this page, is a ten-minute drive from my apartment. If there are more people to interview, they are most likely here, or at least their descendants are; my new friend Russell lives in a nearby suburb. The modern Sister Kenny Rehabilitation Institute is (or was, but more on that later) still operating in the Twin Cities, and how much they might be able to tell me of what I want to know remains to be seen.
I knew I was coming here for a reason. But I didn’t realize it wasn’t any of the ones I’ve listed. I didn’t realize that what I’d find in this new home was something I never knew I was looking for, in the midst of a landscape almost entirely divorced from the map I followed to get here.
The first time I ever came to Minneapolis—this city itself, not its wayward brother St. Paul, where I spent research weekends two blustery Januaries in a row—was the middle of this last April. It was the trip on which I found the place I live, when after a long day of frustration and disappointment I stepped into my new living room and asked, “Where do I sign?” But the trip wasn’t supposed to focus on the hunt for an apartment, which, even with my lease in Chicago rapidly running down, felt more like a lark than anything else. I was here for something on the surface very different, but equally dear to my heart: a yoga teaching seminar with the brilliant Matthew Sanford, whose work I’ve admired ever since I found out about it last year.
I got my yoga teacher training certification about a year ago, at the fitness-focused studio where I practiced in Chicago; it seemed like a good opportunity, and a good next step for something that had become incredibly important in my life. I have always lived amidst deafening noise, struggling with anxiety and a chronic lack of confidence, and learning to breathe through yoga infused both my personal and creative lives with new energy, new hope. It was an arena where I thought I might find a deeper connection between myself, and the things inside my head, and other people, and the outside world, all spaces segregated inside me by improbably high walls. But before long I realized I didn’t have the time in my life, or any real longing in my heart, to teach conventional yoga. Leading the Spandex-clad denizens of Wrigleyville through asanas—the fancy word for poses—meant mostly to tone a part of their body with a similar name, was not the personal development I needed.
Matthew Sanford sometimes teaches yoga to people who wear Spandex, and care how they look from the rear. (I know because I’m one of them.) But he also teaches “nontraditional” yoga to people with disabilities—trying to bring to their lives not just the traditional benefits of yoga (mindfulness, calm, self-reflection, and, yes, fitness) but also something else, something bigger. A sense of their bodies as intrinsically whole, and intrinsically valuable, still beautifully connected to and conversant with their minds, whatever their practical limitations or neurological sensations might be. And he does it all from the wheelchair he’s lived in since he was thirteen, his world transformed instantaneously by a car accident.
 The world inside my head softens, when someone speaks directly to my heart. Just reading about Matt’s work melted me, and I knew right away that that was what I wanted to be involved with. The practical challenge of figuring out how to adapt the essence of poses without losing what they try to tell us about the way we exist in the world (“teach the experience,” as Matt puts it), and the subtler challenge of really being with someone as you go through that together. The challenge of real presence.
The world inside my head softens, when someone speaks directly to my heart. Just reading about Matt’s work melted me, and I knew right away that that was what I wanted to be involved with. The practical challenge of figuring out how to adapt the essence of poses without losing what they try to tell us about the way we exist in the world (“teach the experience,” as Matt puts it), and the subtler challenge of really being with someone as you go through that together. The challenge of real presence.
I took his first training session, like I said, in April, and then the follow-up, second-level program in May. What happened inside those light-filled rooms was amazing to me, and unlike so much else in life it existed with all the superfluity stripped away. This is real, Matt kept telling us—the teacher trainees, and his students, too. This is real life.
And I thought, yeah.
Because it’s the same way I feel about this project, and my novel, too, and the parts of my personal life that I hold the most dear. It speaks to the same impulse as the concept of art, and the sanctity of language—which, for me, is just the most convenient stand-in for the idea of honest communication in general. To put one’s hands on a yoga student, or to sit with someone as they confide a transformative story, or write the story of something that never happened, but could have, and share it with someone who understands—that is the closing of a chasm, the bridging of a gap. It is a stretch toward truth by two parties who are both interested in finding it, rather than avoiding it, for fear it might feel uncomfortable.
Matt teaches his adaptive classes at a place called the Courage Center, a facility with both in- and outpatient clients, working to help those with disabilities live more independent lives. And in a partnership that seems to have rocked the local healthcare world significantly, but that I had managed not to hear about until I got here, it was recently absorbed into one of the local hospital systems—the same one that manages the modern Sister Kenny Institute. Neither one will exist any longer independent of the other. And what that meant didn’t hit me until I filed the paperwork to assist in Matt’s class, and got an e-mail back from the volunteer liason at the newly established conglomeration: “Volunteering at Courage Kenny Rehabilitation Institute.”
I came here in part to be near the Institute, which I hear is still doing pretty remarkable work. But I never imagined I’d work there, or in the place that it’s becoming: a place sort of sentimentally near to my heart, which is both new and old and at a crossroads. Kind of like me.
One of the things I love about the Kenny story, and that of the Kenny Institute specifically, is the sense of cohesion it provided for the people who lived there. The hospital’s philosophy gave the patients a framework for understanding the world and their place in it, and whether and how what had happened meant that had to change. It gave them a way to weld everything together, to take a blast furnace of confusion and frustration and anger and put it to work. And that insistence on wholeness of body and soul, on not just picking up the pieces but taking the time to fit them together into a life that made sense, was everything.

I write about wholeness a lot, and spend a lot of time reflecting on it, but it’s something I’ve never really had. The welded life I love so much is one I’ve never lived. The things that I loved, and the different aspects of the person I wanted to be, and the concerns that I always thought were important, never had a chance to manifest all at once. I could do a handful of things at the same time, and if something crucial was missing, I would go looking for it when something else changed, or I found more time, or things weren’t quite as difficult. When I was less anxious about how people might see me, or what they might think, if my carefully curated worlds collided.
But it isn’t true. The realization came suddenly, and hard, in this new living room: that the day when things are easier, or I have more time, or fewer preoccupations, is never going to come. There are a million moments of right now in a lifetime, each one different, and weighted down with context. But right now is the only thing that there will ever be.
I was eighteen years old when I moved to Chicago. I knew a lot about what, and who, and where, I didn’t want to be. (An Apple computer salesperson, stuck in the suburbs of Baltimore, four years out of college and without any idea where to go, or whether I might ever fit in.) But I never felt truly empowered to choose something different. I never found a community where I could be myself, or people with whom I felt compelled to get seriously involved. I yearned for independence: the feeling of independence, of agency, which is far more ephemeral than people realize. I lived on my own for years without ever feeling empowered to drive my own life in the direction I felt it was really meant to go.

I spent a long time shy and embarrassed about my writing, about my past, my philosophy, my life. I still haven’t talked very much about my background, but I’m planning to; I want you to know me, and why I’m doing this, as well as you come to know the people who populate the sepia picture I’m painting. I don’t want to write myself into my own book; the end product this blog teases is about Elizabeth Kenny, and the people she helped (and some of those she couldn’t), not about me. But talking about the process is inevitably a way of talking about myself, especially now that my thousand shattered lives are sharpening, finally, to a single point.
I lived a yoga life, before. A life as a fiction writer, and a separate life as someone embarking on a research project that seemed impossibly audacious, given my background: an undergrad degree in biology didn’t seem legitimate enough to speak on such a momentous topic, and my five years in the pediatric ER of Johns Hopkins Hospital felt like an inadequate explanation of my interest in medicine. I never talked about my writing with strangers. I’ve lived lives in secret, and lives that were highly visible but not quite true. I’ve never spent much time trying to fit into others’ expectations, but I have spent long years being wistfully misinterpreted by the people around me. I have tried silence, and I have tried angry, self-righteous defiance, but I have never tried acceptance. I have never stood still in the midst of myself and acknowledged the things about me that are unchangeably true, or honestly tried to escape the traps I fell into by accident, and than stayed in out of fear and inertia, the ones filled up with easy, painful lies.

What does it mean to embrace being lost, when it takes even more bravery to admit to being found? There is no agreed-upon scorecard in life, at least not one any useful number of people will agree on; you will never know if you’ve “won.” The only judge worth listening to is the barely audible voice inside your head, whispering breathily that you’ve done the right thing, and it’s all too easy not to listen. Because what if you’re wrong? What if it’s made-up, and this thing seems so wonderfully laden with potential just because it happens to be better than the terrible situation you’d been mired in before? What if you are merely the victim of a fresh landscape, and the wishful thinking that comes along with it?
What if it doesn’t matter? Who the hell cares? Wishful thinking is a cynic’s synonym for hope. Perception is reality. And we write our own stories every minute we’re alive.
Everything is different here. The weather is different: unseasonably cool and sticky, and unremittingly gray (unusually, the locals promise), with a ceiling of clouds that peel like wallpaper. The people are different: they move more slowly than I’m used to, and talk more sharply, about places and things whose names I don’t know. The neighborhood is another world, with its quiet residential streets and quilted flower gardens, sitting apart from the vintage shops and bike vendors and dive bars on Lyndale. There are as many restaurants in my entire neighborhood as there were in the five blocks around my old place. Even more of the twentysomething hipsters stalking down the streets sport slashes of neon color in their short-cut hair, but they look more out of place than they did in Chicago. More ostentatious, but quietly so, circumscribed in their defiance.
I am different here, but not because of any of that. Because when everything you know falls away, your first instinct is to do everything in your power to find those things again, and snatch them back, keep them safe. And the liberation in realizing that maybe they aren’t the ones you need after all—that is beautiful, and terrifying. And something it’s going to take a lot longer than three weeks to sort out.
My journey is far less dramatic than that of the kids that I write about. I have not been blindsided, traumatized, or terrorized (at least not in the short term); if my world has been upended, it has been by something that at least on the surface I chose. But that doesn’t mean I know exactly where I am, or have a good grasp on where I’m going, or that keeping the faith is always—or ever—simple. It’s a positive change, this one that I find myself so unexpectedly facing, but it is one I feel unprepared to handle, even as I hope to use it as a springboard to the kind of wonder I’ve never successfully held. I’m hoping I can learn from them—Kenny’s kids, the ones that I feel I’m watching over, now, in this place with so many memories, and so many echoes of beauty. With fortitude, and a little bit of luck, I’m here not just to tell their story, but to follow their example.
I am definitely still a little lost here. But sometimes, when you’re lucky, in being lost to the world, you get a chance to find yourself.