Tags
“‘Bill’ Stanley William / Willis Bell (??)”
That name is written not far beneath Elizabeth Kenny’s, in my roster of important figures in this absurdly crowded story. So far, I’ve talked only about Kenny herself, and about her patients—and, in my last post, about myself—but there are dozens, if not hundreds, of others who figure into this story. They are nearly as vibrant and dynamic as its central character, but were afforded nowhere near as much press coverage, and finding ways to get to know them has proven both delightful and infuriating.
This story is vast, almost beyond my ability to see it all at once, force a wide and ever-changing vista into a single frame. It’s yet another part of what I love about it: its enormity, and the delight I take in the knowledge that each one of the many thousands of people who passed through the Kenny Institute, for a week or a month or a year, came away with a different impression of what the place was and exactly who the people were that lived and worked there.
Because it’s not what a thing really is that we see, that we remember. It’s what it means to us.
The physical therapist with that heavily annotated name is one of my favorites: one of the most interesting, and so far one of the most enigmatic. It isn’t just that the names on his paperwork don’t match up (though they don’t, always, with William/Willis the main point of contention). It’s that he seems to have used different names with different people—and it’s that one small quirk that has me curiously transfixed.
It was while I was talking to my interviewee Russell, who fell ill in the summer of 1940, that I figured this out: I’d asked him about the people who cared for him other than Kenny, hoping to draw out some of the names I already knew. “[S]he had one male and one female nurse that was on her staff, Australians,” he said, but he couldn’t remember their names.
The girl was probably Mary, I told him, or else Valerie: Kenny’s adopted daughter and protégé, and her favorite physical therapist, respectively, both of whom accompanied her from Australia. The boy’s name was almost certainly Bill, another therapist she’d trained—someone I’d heard stories about, who all of the kids seemed to adore. I’d read a lot about Bill, and I was confident that this was Russell’s guy. Did any of that sound familiar? I asked.
It didn’t. Not then. But a few minutes later, he told me about this “orderly” he’d worked with almost constantly, someone who helped him with his treatments and carried out his exercises. Stan, he said, thoughtlessly. Sliding out, the way things do, from dark corners of memory too cluttered to retrieve anything from when you rifle through them in the light.
And something went off in my head.
Stan. Stanley? Stanley William? Bill?
I’d read people’s recollections about the somewhat unfortunately named Bill Bell, but never any—at least, none that I recall—about Stan. And yet it’s obvious that the man Russell spoke of with such mischievous warmth in his voice was the same one who’d watched over so many others in their most fragile and brilliant moments: outgoing and deadpan and subversively indulgent, with the same Aussie drawl Kenny had.
Stanley et cetera Bell was one of the Kenny Institute’s first staff members—he started working for Kenny in the States in 1940, and the Institute wasn’t dedicated until December of 1942—and to all appearances one of its most beloved. Kenny summoned him from Australia the instant she was ensconced in Minneapolis; she had trained him in physical therapy at a clinic she ran in Queensland, and the two had worked closely together for his entire career to date. As apparently skilled and authoritative as anyone else on Kenny’s staff, Bill/Stan also had a bit of a “good cop” reputation, contrasting with the women’s more severely expressed expectations. “Stan and I got along like a million bucks,” Russell told me, grinning, and it was clear that to a lost, lonely kid looking for guidance, that meant everything.
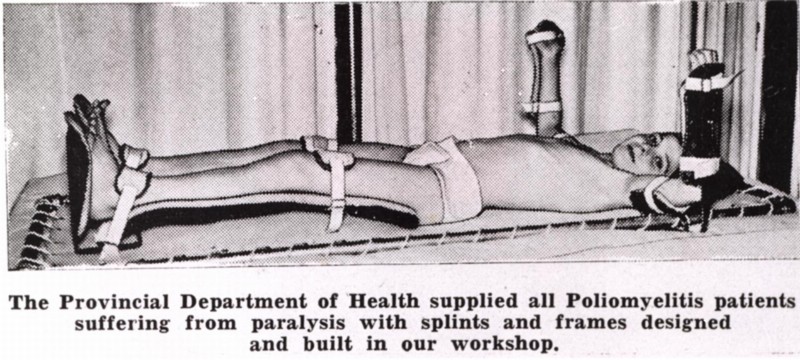
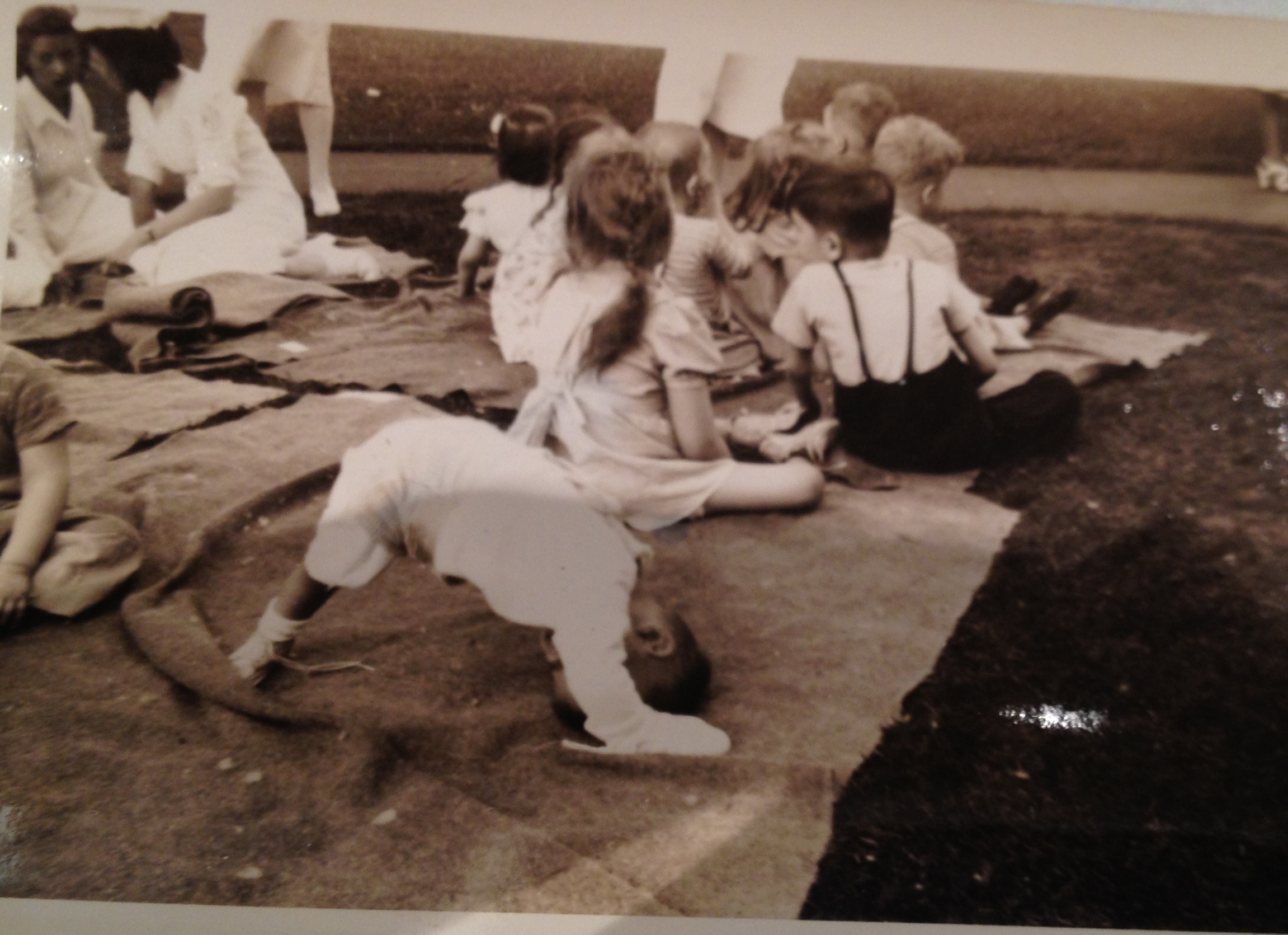
 The Kenny Institute, as it was in the 1940s, was, and still sometimes is, accused of being a “cult of personality”—but no hospital serving nearly a hundred people as long-term inpatients, and two or three times that during certain epidemic swells, could operate on the strength of a single individual, no matter how formidable she might have been. Sister Kenny’s ethos permeated the place, but it’s the auxiliary staff former patients recall most vividly: the people they saw every day, sometimes more than once. (Sometimes an exasperatingly large number of times.) The nurses. The “packers” who swathed their bodies in hot wool blankets to ease their cramps. And the therapists, who coaxed them so slowly and steadily back to life. People who knew them better than they knew themselves, at least for that brief breath-held moment in time, who bore witness to their tears and shared in their triumphs, and were both the cause and the cure of their pain.
The Kenny Institute, as it was in the 1940s, was, and still sometimes is, accused of being a “cult of personality”—but no hospital serving nearly a hundred people as long-term inpatients, and two or three times that during certain epidemic swells, could operate on the strength of a single individual, no matter how formidable she might have been. Sister Kenny’s ethos permeated the place, but it’s the auxiliary staff former patients recall most vividly: the people they saw every day, sometimes more than once. (Sometimes an exasperatingly large number of times.) The nurses. The “packers” who swathed their bodies in hot wool blankets to ease their cramps. And the therapists, who coaxed them so slowly and steadily back to life. People who knew them better than they knew themselves, at least for that brief breath-held moment in time, who bore witness to their tears and shared in their triumphs, and were both the cause and the cure of their pain.
It was the most intimate relationship many of them had ever had—not just the children, but, by all accounts, many of the adults as well. It amazes me how openly Kenny patients talk about their doctors and therapists—not just in retrospect, but in things they wrote while they were still in the hospital, or shortly thereafter. They seem to have talked to them just as candidly: without any of the frightened reverence I’m used to seeing in the face of such an authority gap, they tease and question them even as they look to them for guidance. It’s respect, and well-earned, not intimidation.
It’s like I wrote in the last post: this is real life. With all of the extraneous distraction, and all of the social nicety, stripped away. If you didn’t have the luxury of hiding from it, it was good at least to have someone with whom to share, and these were the people they could trust. And the patients—some of them, anyway, when they were ready—plunged into this highly unusual dynamic with an abandon and a sense of freedom they didn’t seem to feel anywhere else. You weren’t supposed to talk about it—about polio, about your fears, about much of anything at all; recollections of interactions with family and friends frequently emanate squirming discomfort. But this specific relationship, between the Kenny patients and their therapists, that you might expect to be so fraught with expectation and fear, is both ocean-deep and light as air.
And they entrance me, coming to life on these old and crinkled pages. It’s uncanny, in a way, to come away with such a strong impression of an individual—not just the mysterious Mr. Bell, but so many of these people, the ones who show up all the time and the ones I’ve “met” just once or twice—without actually knowing anything about them. I have a copy of a card with Bell’s credentials on it—but most of Kenny’s resume was faked, so I have a hard time believing his is wholly straightforward. He spent some time in the military starting in 1945, but how that came about, and why, as far as I can tell, he never returned to the Institute, remains a mystery. He was married, with at least two children, but I don’t know anything about his family besides that they existed.
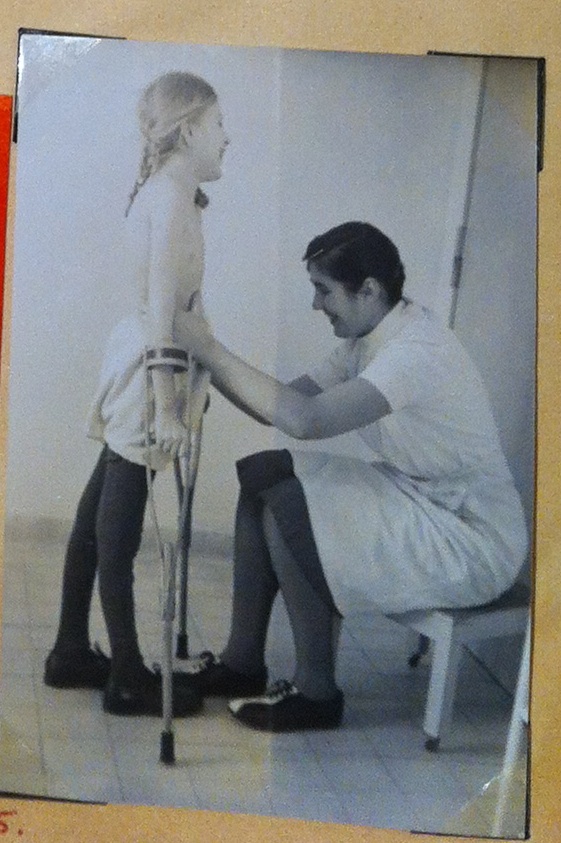
 The only thing about Bill/Stan Bell I don’t have any trouble figuring out is why he was so thoroughly beloved. The first story I ever read about him was relayed by a man named Robert Gurney, in an interview for the book Polio’s Legacy. Robert called him Bill. He called him Bill, and he spoke about the winter of 1940, and learning to walk again: seventeen years old at the time, Robert insisted he couldn’t do it, but his technician felt otherwise. After a couple unsteady laps around the therapy table, Bill announced that Robert, with Bill’s help, was going to walk back to his room. This plan seemed difficult to protest, so off they went, until one of Robert’s friends noticed him walking alone and called out congratulations; as it turned out, Bill had stopped to “[talk] to a couple of pretty nurses,” and Robert had inadvertently kept going without him. As soon as he realized what had happened, Robert promptly wavered and fell, but he tells it as a deeply happy story, infused with nostalgia, tinged with gratitude.
The only thing about Bill/Stan Bell I don’t have any trouble figuring out is why he was so thoroughly beloved. The first story I ever read about him was relayed by a man named Robert Gurney, in an interview for the book Polio’s Legacy. Robert called him Bill. He called him Bill, and he spoke about the winter of 1940, and learning to walk again: seventeen years old at the time, Robert insisted he couldn’t do it, but his technician felt otherwise. After a couple unsteady laps around the therapy table, Bill announced that Robert, with Bill’s help, was going to walk back to his room. This plan seemed difficult to protest, so off they went, until one of Robert’s friends noticed him walking alone and called out congratulations; as it turned out, Bill had stopped to “[talk] to a couple of pretty nurses,” and Robert had inadvertently kept going without him. As soon as he realized what had happened, Robert promptly wavered and fell, but he tells it as a deeply happy story, infused with nostalgia, tinged with gratitude.
“Henry [the friend] was laughing so hard he was crying,” Gurney says, “and I was just sitting on the floor laughing. But from then on, I walked.”
The interview is eight or nine pages long, and only one of them deals with this incident, much less Bill himself. But I came away from those bare sentences with a distinct impression of who this person was and how he thought (though I still can’t decide whether the detour to chat up the nurses was an actual lark or just a ruse). I feel like that’s the opposite of what usually happens, like I’m getting to know these people inside out: it’s so easy to accumulate semantic details about a person—what do you do, where are you from, where’d you go to school?—and so hard to actually learn anything about who they are. But these people come across as so raw, so earnest, so inside-out, that it’s hard not to see them right away. You see them in their letters, in their memos, in the stories that others tell about them, so enthusiastic and conspiratorial: the way they really were, in the day-in and day-out of a job both unforgiving and unfathomably rewarding.
That’s why I’m so curious about the name change. About why Russell talks about Stan, and Robert reminisces about Bill, when they met him the very same summer, a span of time in which you expect there to be a united front. Maybe it’s an odd thing to have latched onto so tightly, and with such insistent curiosity. But names have a literally mythological power, and changing them is more than just semantic, because your name tells you—you, not just the rest of the world—so very much about who you are. You can be a different person, with a different name. Even if they both belong to you, and neither one is a “disguise.”
I know because I changed my name, a little less than a year ago, one little piecemeal introduction at a time, from something that merely belonged to me to something that was mine. I’d been Tori since I was born, an abbreviation of a given name I claimed to hate, and that even my parents never meant to call me aloud: too regal, too stuffy. I was so stubborn about it that it says Tori on my university diploma. But about a year ago, with the world swirling around me, I started wondering if that was the person I felt like—or the person I wanted to be. I started wondering about Tori on the cover of a book. And then, one day, with a small and instantaneous thrill of transgression: Hi. I’m Victoria.
I love this “new” name. Victoria is who I chose to be. And there are many people in my life now who know me only that way: when my yoga teacher Matt calls me out in class, it is Victoria he gently chides; Victoria is the name at the top of this page. It startles me when I swipe my loyalty card at the chain café I’ve eaten at practically every other day since I was a teenager, and when my order comes up they call out, “Tori?” And yet, sometimes, for reasons I can’t even fathom, a department store salesperson will ask my name, and I’ll chirp the shorter version—not because I forget, for a moment, but because it feels more appropriate. Even though most of the time I cringe, unfairly, when I see that worn-out word, the old name, a relic of a person I’m relieved to no longer be.
Sometimes a name is just a name. But sometimes it’s a threshold.
So that’s a moment—a pair of them, in fact—I wish I somehow could have witnessed: whatever the space was between Stan/Bill’s two introductions, and whatever spontaneous impulse triggered the change. Maybe different people seemed to need different things. Maybe different contexts brought different levels of comfort. Maybe he was still trying to figure out who he was going to be in the U.S., and whether that was any different from the person he had been back in Australia. Maybe it’s nothing. Maybe he went by both names as a matter of course, and the kids he worked with picked their favorite as shorthand. Maybe one of the boys whose stories I’ve mentioned couldn’t remember at all, and paperwork or an interested family member supplied a name different from the one he used every day. Or maybe there was somebody else named Bill, or Stan, on one of those wards, and that someone was unusually protective of his name.
 I probably won’t ever know. Not that particular detail, so specific, and so likely inconsequential, no matter how much I want to read into it. I’ll keep gathering stories, the ones about Stan and the ones about Bill, and I’ll figure out the truth, if not about the name, then about the things that happened, and I’ll line them up for you: in the proper order, and with proper annotation, and with as little of the conjecture I’m making right now as possible. But the writing of this book is about more than just that, and that’s one of the things I’ve been grappling with over the last few weeks, writing and thinking such personal things.
I probably won’t ever know. Not that particular detail, so specific, and so likely inconsequential, no matter how much I want to read into it. I’ll keep gathering stories, the ones about Stan and the ones about Bill, and I’ll figure out the truth, if not about the name, then about the things that happened, and I’ll line them up for you: in the proper order, and with proper annotation, and with as little of the conjecture I’m making right now as possible. But the writing of this book is about more than just that, and that’s one of the things I’ve been grappling with over the last few weeks, writing and thinking such personal things.
I have no idea where I heard this story (yet another damning piece of evidence against my bibliographic skills, which before I started this project left very much to be desired), but it bears repeating anyway. Whether this is a yarn about a real place or an urban legend, a kind of artist’s parable, I don’t know, but it goes like this: there was once a little bookstore with only two sections. Over one cluster of shelves hung a sign that read Facts—nonfiction. And over the other? Truth. The fiction section.
When I first heard that little tale, fiction was the only thing I wrote—at least, the only thing I wrote of my own volition, and the only writing I shared with others that didn’t come back with a letter grade attached. I loved the story then, and I love it still, but it sounds different to me, after all these years, because my situation is different now. I write both. And I think about that anecdote now, and I wonder: why choose just one?
There are things in my novel that reference actual reality, but I didn’t put them there because I wanted anyone to learn anything. Fiction sits on the side of truth, at least when it’s doing its job as it should, and no one asks from it anything more than that—which is exactly as it ought to be. But nonfiction, that’s a different animal. There’s an implied derision in that simple word: facts. It conjures a sterility we remember from textbooks, and it’s a legitimate criticism: I am deeply buried in facts, trying to wade through the existing literature on the history of polio, and it can be stifling. I love to read the scientific papers of the time, which have a sort of sly elegance and cleverness the modern journals I studied in college totally lack, but the secondary sources, the academic tomes, are dry and impersonal in a way that feels to me almost heart-wrenching.
It’s important to provide accurate reportage, and a worthy accounting of the truth. But I love this story because it’s about people. People, and their lives and hearts and minds. People’s families, people’s memories, people’s heritage and hopes. Writers of nonfiction shy from those things, too often. Hoping, perhaps, that people will be able to extract the appropriate feelings from an endlessly unspooling reel of names, dates, and featureless interactions, or perhaps just afraid of accusations of bias or inaccuracy. But that’s the one thing the little bookstore parable has right: facts aren’t, intrinsically, connected to truth. The people I’m writing about deserve better than to be reduced to sweeping generalizations and gut-wrenchingly vague statistics. And they also deserve for someone to tell their stories correctly.
That’s why I look for those signatures, on Bill Stanley Willis William Bell’s letters, and why I pore so carefully over the accounts of those he worked with. Because I think that facts can tell us the truth, if we understand that there’s more there to speak than mere procedure. I love the way the whole world talks to itself: the way the specificity of these anecdotes becomes, always, universal, and the way semantic details can reveal intimate and tender emotions. It’s curiosity about people that leads me to recognize the gaps in my factual, biographical knowledge. It’s because I want explanations for the events and quotations and little quirks of behavior that allowed this thing, this crazy improbability that was the Kenny Institute, to happen the way that it did. And the discoveries I’ve made that way are what convinces me that even good math can add up to something greater than the sum of its parts.
That this story is so emotionally clear and so factually opaque is both its glory and its misery, and I’ve been sledgehammered by that a dozen times since I’ve gotten to Minneapolis. The folders and folders and folders of misfiled letters and papers shuffled like cards in a poker shoe over at the Historical Society are heart-stoppingly overwhelming, and the photographs and jokey newsletters written by Kenny’s patients feel like coming up for air. But I fight through the one to shore up the other. Because—like I’ve said before—I want people to see this thing the way that I do, and I know that means giving you something to latch onto that makes sense. Something that’s real. Something that’s true.
However you choose to interpret that, and whatever name it goes by.